
Introduction of Aspergillus
Table of Contents
The genus Aspergillus has more than 180 species, among them, 38 are responsible to cause disease (able to grow at 37◦C. They are common in the environment. Aspergillus species are emerging pathogens which are ubiquitous molds that infect immunocompetent ( rarely) and immunocompromised patients ( mainly). The symptoms are diverse and range from allergic reactions, bronchopulmonary infection, and bronchitis, to invasive aspergillosis. A. fumigatus is the main opportunistic pathogen. Other medically important species are Aspergillus niger, Aspergillus flavus, Aspergillus terreus, and Aspergillus nidulans.
Rate of growth
- Usually rapid
- Mature within 3 days
- Only a few species are slower growing.
Classification of Aspergillus
- Kingdom: Fungi
- Division: Ascomycota
- Class: Eurotiomycetes
- Order: Eurotiales
- Family: Trichocomaceae
- Genus: Aspergillus
- Species: Aspergillus fumigatus
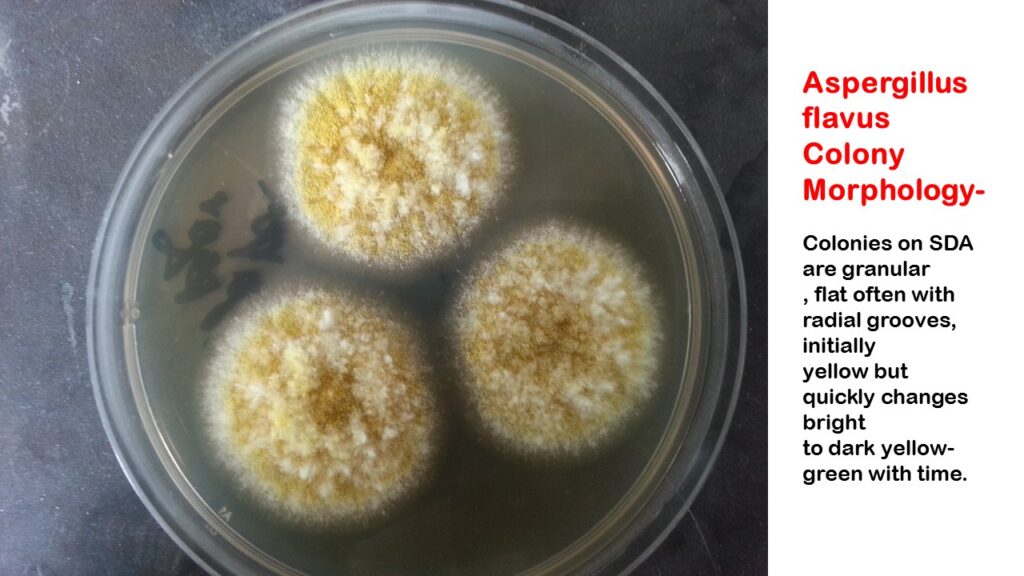
Colony Morphology of Aspergillus
Macroscopic morphology
- The surface at first white then any shade of yellow, green, brown, or black depending on the Species
- Texture velvety and cottony
- The reverse is white, golden, or brown
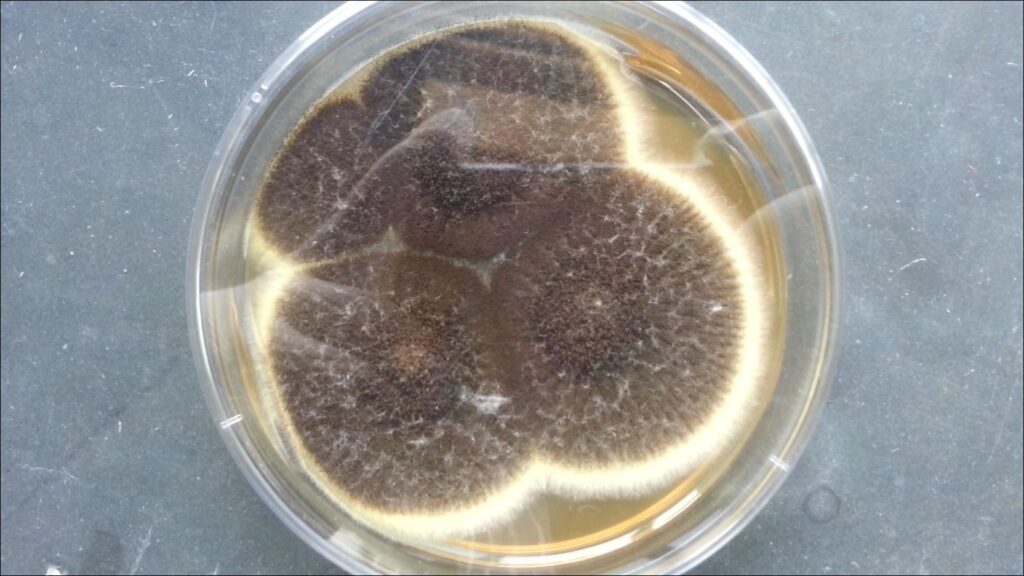
Aspergillus fumigatus colony characteristics on SDA

Microscopic morphology
- Septate hyphae(2.5-8.0 µm)
- Unbranched conidiophore arises from foot cells
- The conidiophore is enlarged at the tip forming a vesicle.
- Vesicles are completely or partially covered with flask-shaped phialides.
- Phialides may develop directly on the vesicle(Uniseriate form) or be supported by metula (biseriate form).
- The phialides produce a chain of round conidia(2-5µm).

Aspergillus fumigatus in LPCB showing conidia, conidiophores and phialides

Characteristics of common pathogenic Aspergillus species
| Species | Conidiophore length ( mm) | Conidiophore length ( mm) | Phialides | Conidia Diameter (µm) | Conidia color |
| Aspergillus niger | 1.5-3.0 | 45-75 | Biseriate | 4.5-5.0 | Black |
| Aspergillus fumigatus | <0.3 | 20-30 i.e. Only the top half conidiogenous | Uniseriate | 2.5-3.0 | Green or bluish green |
| Aspergillus flavus | <1 | 25-45 | Uniseriate or biseriate | 3.5-4.5 | Yellow to green |
| Aspergillus terreus | <0.25 | 30-50 | Biseriate Compactly columnar | 1.5-2.5 | Cinnamon-buff to sand brown in color with a yellow to deep dirty brown reverse |
The genus Aspergillus – important to humanity
On the negative side
They cause invasive and allergic diseases in humans and other animals. e.g. A. fumigatus.They cause plant and food spoilage and produce mycotoxins. e.g. A. flavus and A. parasiticus
On the positive side:
- Composting: Well-established model organism in cell biology and genetics: A. nidulans
- food production: enzymes and organic acids: A. niger
- East Asian foods: A. oryzae and A. sojae
- pharmaceuticals: echinocandins-A. nidulans and A. sydowi
- lovastatin-A. terreus fumagillin: A. fumigatus
Life Cycle

Pathogenesis
Aspergillosis is caused by inhalation of conidia or mycelial filaments which are present in the decaying matter, soil or air. When the host defense is compromised, aspergillosis may develop. The common clinical forms of systemic aspergillosis are as follows-
Respiratory Disease
Bronchopulmonary aspergillosis: The organism grows within the lumen of the bronchioles, which may be occluded by fungus plugs. Some patients may expectorate mucus plugs containing fungus.
Aspergillus asthma: Allergy to aspergilla may occur in atopic individuals following inhalation of spores of aspergilli.
Aspergilloma: It is also known as a fungus ball. The fungus colonies in pre-existing pulmonary cavities such as tuberculosis or cystic disease.
Invasive aspergillosis
It is also called disseminated aspergillosis and it occurs in severely immunocompromised hosts. The organism first establishes in lung tissue and then disseminates to involve other organs, particularly the Brain, kidney, and heart.
Superficial infections
Sinusitis: Inflammation of sinus and causative agents are A. flavus and A. fumagatus.
Mycotic Keratitis: Causative agents are A. flavus and A. fumagatus.
Otomycosis: Mainly Aspergillus niger
Classification of Aspergillosis

Immunosuppression and Infection
- Inhalation of aspergillus spores is a common daily occurrence. A healthy immune system would normally remove the spores and no symptoms or infection would occur.
- In individuals whose immune system may be suppressed either because of illness e.g. AIDS, cancer, diabetic patients, or drugs, spores may germinate, and resulting tissue or systemic aspergillus invasion can result
- Individuals with allergies such as asthma can also be vulnerable to aspergillus disease.
Interaction of Aspergillus with the Host
A unique microbial-host interaction-

Disorder of the immune response-Concept
Changing incidence of fatal invasive mycoses in non-HIV patients in the USA

Invasive pulmonary Aspergillosis

Predisposing host factors and immunopathogenesis of invasive, saprophytic, and allergic bronchopulmonary aspergillosis
| Patient populations | Predisposing host factors | Clinical and histological features |
| Acute leukemia, myelodysplastic syndrome, aplastic anemia, and other causes of marrow failure | Neutropenia | Hyphal angioinvasion with vascular thrombosis and tissue infarction; scant inflammatory response; may evolve to cavitation |
| Allogeneic HSCT after neutrophil recovery | Immunosuppression for GVHD (e.g., corticosteroids, T-cell-depletion; tumor necrosis factor- inhibition) | Inflammatory fungal pneumonia; angioinvasion with coagulative necrosis resembling aspergillosis classically associated with neutropenia may occur |
| Solid organ transplantation | Immunosuppression to prevent allograft rejection | May range from acute inflammatory pneumonia to chronic necrotizing aspergillosis; in lung transplant recipients, Aspergillus tracheobronchitis may affect the anastomotic site and cause dehiscence |
| Advanced AIDS | CD4+ T-cell count generally < 100/ul; immunocompromising conditions (e.g., neutropenia) and other opportunistic infections often co-exist | Acute to slowly progressive necrotizing pneumonia; variable histological findings: neutrophilic infiltrates, vascular invasion, walled-off abscesses, and cavitation occur; extrapulmonary dissemination observed |
| Chronic granulomatous disease | Defective NADPH oxidase | Varies from acute pneumonia to slowly progressive disease; pyogranulomatous inflammation without hyphal vascular invasion or coagulative necrosis; “mulch pneumonitis” is an acute hypersensitivity response to a large aerosolized exposure |
| Pre-existing structural lung disease (e.g., emphysema, prior cavitary tuberculosis) | Comorbid conditions, including diabetes, malnutrition, inhaled and low-dose systemic corticosteroids | Chronic necrotizing pulmonary aspergillosis: slowly progressive invasive fungal pneumonia with inflammatory necrosis |
| Aspergilloma | Pre-existing structural lung diseases, e.g. bronchiectasis or prior cavitary tuberculosis | “Fungal ball” composed of hyphal elements in the pre-existing cavity; erosion into adjacent vessels can cause life-threatening hemoptysis; surgical resection is the definitive treatment for hemoptysis from aspergilloma |
| Allergic bronchopulmonary aspergillosis (ABPA) | Allergic disease; can be an important complication of cystic fibrosis | Airway plugging with hyphae, mucous, and inflammatory cells; hyphae do not invade lung parenchyma; airway and lung hypereosinophilic inflammation; goblet cell hyperplasia; central bronchiectasis in advanced disease |
Laboratory Diagnosis
Specimen: It also depends on the types of infection sites. However, the most common specimens are sputum, bronchoalveolar lavage (BAL), biopsy, and blood.
Direct Microscopy: KOH mount of sputum and BAL helps to identify fungal elements like spores and hyphae.

Culture: It is highly sensitive than microscopy but the time is taken procedure. Organisms can be cultivated on fungal culture media. They are fast growers so they can be cultivated within 4 days.
LPCB Tease Mount Preparation: Etiological agent/ Aspergillus can be phenotypically confirmed via this LPCB tease mount preparation.

Molecular Test (PCR): It is also a more rapid assay than culture and most sensitive than other techniques (microscopy and culture. It is also a confirmatory test of fungi.
Histopathological Examination: Biopsy specimens are stained and examined for fungal elements.
Other (Radiological) examination: Imaging test like X-ray and CT-scan helps to find out a fungal mass (aspergilloma) that is the marker of invasive aspergillosis and allergic bronchopulmonary aspergillosis.
Treatment
Aspergillosis treatments vary with the nature of the disease. The possible treatments are-
- Observation
- Application of oral corticosteroids
- Antifungal medications: The choice of antifungal drug for invasive pulmonary aspergillosis is voriconazole and another drug Amphotericin B may also be used.
- Surgery: It is useful since antifungal drugs don’t penetrate an aspergilloma properly, surgery to remove the fungal mass is the first-choice treatment when an aspergilloma causes bleeding in the lungs.
- Embolization: This is a radiological temporary procedure that stops lung bleeding caused by an aspergilloma.
Prevention
Aspergillus spores can not be avoided in breathing because the fungus is ubiquitous in the environment. For people who are immunocompromised or weakened immune systems, there may be some ways to reduce the chances of developing a severe Aspergillus infection.
- Protect yourself from the environment-Use masks, wear shoes, long pants, and a long-sleeved shirt when you are gardening, doing yard work, or visiting wooded areas. Don’t forget to wear gloves when handling materials such as soil, moss, or manure.
- Antifungal medication: An organ transplant or a stem cell transplant patient is at high risk for developing invasive aspergillosis. In such cases, clinicians may prescribe medication to prevent aspergillosis.
- Testing for early infection: Patients who are at high risk may benefit from blood tests to detect invasive aspergillosis.
Keynotes
Early diagnosis of invasive aspergillosis is important because of-
| Treatment started | <10 days | >11 days |
| Mortality rate | 40% | 90% |
| Source | -Von Eiff et al, Respiration 1995;62:241-7 |
- Aspergillosis is not contagious since it can’t spread between people or between people and animals from the lungs.
- Thrombocytopenia may limit the ability to perform invasive procedures.
- In contrast to adults, children with invasive pulmonary aspergillosis frequently do not manifest cavitation or the air crescent or halo signs.
- Culture correlation with KOH mount examination is important because aspergilli are common laboratory contaminants.
- 6 consecutive morning sputum samples are required out of which should show the same fungi in 50% of samples.
Further Reading
- https://www.cdc.gov/fungal/diseases/aspergillosis/index.html
- https://www.hindawi.com/journals/scientifica/2013/459405/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3326383/
- https://cmr.asm.org/content/22/3/447
- https://www.clinicalmicrobiologyandinfection.com/article/S1198-743X(18)30051-X/fulltext
- https://err.ersjournals.com/content/20/121/156
- https://patient.info/doctor/aspergillosis
- Textbook of Medical Mycology, Jagdish Chander
I loved your blog. Great.
cheap cialis online pharmacy
citalopram for depression
Canadian Pharmacy 24h Best pharmacy in canada Cheap viagra for sale black cialis 5 mg cialis generic india