
Introduction of Coomb Test
Table of Contents
Direct Coomb Test (DCT) is a type of Coomb test also called the anti-globulin test. It is of two types-Direct Coomb’s test (DCT) and the Indirect Coomb’s test (ICT). DCT uses to detect sensitized red blood cells (RBCs) while ICT detects the presence of ‘incomplete’ Rh antibodies i.e. IgG antibodies. IgG antibodies are capable of sensitizing RBCs but incapable of causing agglutination of RBCs (hemagglutination). Coomb’s test was introduced by Cambridge immunologists Robin Coomb and his et. al. (Arthur Mourant and Rob Race) in 1945.

Principle of Direct Coomb Test (DCT)
Direct anti-human globulin test is used to detect the sensitized red blood cells in particular Immunoglobulin gamma (IgG) and Immunoglobulin meu (IgM) that is present in patient red blood cells.
Requirements for DCT
Following equipment and reagents are needed to proceed direct Coomb’s test.
- Refrigerator
- Tabletop centrifuge
- View box/Microscope
- Water bath
- Anti-human globulin (AHG)
- Normal saline
- Glass test tubes (10 × 75 mm)
- Test tube rack
- Pasteur pipette or micro pipette
- Marker
- Container for waste disposal
- Tissue paper
- Specimen-Blood-Particularly EDTA is preferred but oxalate, or clotted, citrated whole blood may be used ( the specimen needs to be a fasting sample).
The procedure of the Direct Coomb Test
- Take 3 test tubes and label them as T, N, and P for the test sample, negative control, and positive control respectively.
- Add 2/2 drops of washed patient cells, washed O red cells, and sensitized red blood cells in T, N, and P test tubes respectively.
- Add 1/1 drop of anti-human globulin to all test tubes.
- Incubate at room temperature for 5 minutes.
- Now, mix it and centrifuge at 1000 rpm for 1 minute.
- Gently re-suspend the red cell bottom and examine for agglutination or clumping.
- Observe macroscopically.
- If it is doubtful in macroscopic observation, proceed microscopically.

Result and Interpretation of Direct Coomb Test (DCT)
- Negative control: No agglutination
- Positive control: Agglutination
- Test: Agglutination or no agglutination
- Presence of agglutination or clumping: Direct Coomb Test (DCT) Positive
- Absence of agglutination or clumping: Direct Coomb Test (DCT) Negative
Direct Coomb Test (DCT) Negative

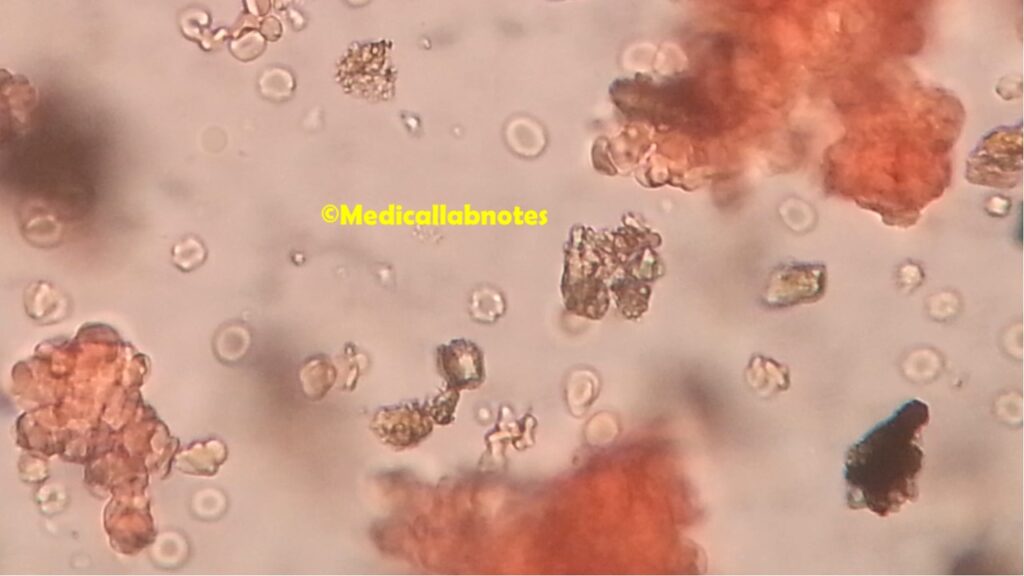
Direct Coomb Test (DCT) Positive
Clinical Significance of DCT
This test is performed to detect sensitized RBCs or anti-D antibodies or other antibodies attached to the red blood cell surface within the bloodstream. This occurs in the following conditions:
- Erythroblastosis fetalis or hemolytic disease of the newborn (HDN): When there is an Rh-positive baby in the womb of a sensitized Rh-negative woman, the antibodies produced in the mother’s serum cross the placenta, and after entering the baby’s bloodstream, these antibodies will attach to the bloodstream, these antibodies will attach to the baby’s Rh-positive red blood cells. These coated ( or sensitized) cells are clumped and removed from the circulations causing hemolytic anemia. When the baby is born, the baby’s blood (cord blood collected from the umbilical cord) is collected and tested for the Direct Coomb test.
- Transfusion reaction
- Drug-induced red cell sensitization
- Autoimmune hemolytic anemia
Keynotes on DCT
- Anti-Rh antibodies are of IgG type that normally do not agglutinate Rh-positive RBCs so anti-Rh antibodies are also known as incomplete antibodies as resistant to ‘complete’ IgM antibodies, which do agglutinate red cells.
- Anti-human globulin (AHG) is also called Coomb’s reagent
- The sensitivity of the test can be increased by incubation at room temperature for 5 to 10 minutes and by re-centrifugation.
- In a simple setup, DCT is performed in test tubes while in the advanced laboratory, it is commonly done using micro-array and gel technology.
- Coomb’s reagent contains antibodies against all four classes of IgG and components of complement (usually C3 and C4).
Introduction of Indirect Coomb Test (ICT)
The indirect Coomb Test is a type of Coomb’s test also called the anti-globulin test. It is of two types-Direct Coomb’s test (DCT) and the Indirect Coomb’s test (ICT). DCT uses to detect sensitized red blood cells (RBCs) while ICT detects the presence of ‘incomplete’ Rh antibodies i.e. IgG antibodies. IgG antibodies are capable of sensitizing RBCs but incapable of causing agglutination of RBCs (hemagglutination). Coomb’s test was introduced by Cambridge immunologists Robin Coomb and his et. al. (Arthur Mourant and Rob Race) in 1945.
Principle of Indirect Coomb Test
Complement proteins, or more often, incomplete antibodies (IgG), connect to the red cell membrane via the Fab part of the immunoglobulin under certain conditions. These cells are referred to as sensitive cells. Red cell sensitization can happen in vivo or in vitro. The IgG molecules attached to red cells are unable to traverse the gap between sensitized red cells separated by their negative charge on their surface, resulting in the sensitized red cells failing to agglutinate. The reaction is completed when Coomb’s reagent is added. The Fab portion of the anti-human globulin molecule (anti-IgG) combines with the Fc portions of two adjacent IgG molecules attached to red cells when the serum is administered to the sensitized cells, bridging the gap between sensitized red cells and causing agglutination.
Requirements for Indirect Coomb Test
The following equipment and reagents are useful to proceed with indirect Coomb tests-
- Refrigerator
- Tabletop centrifuge
- View box/Microscope
- Water bath (for 37°C)
- Anti-human globulin (AHG) or Coomb’s reagent
- Anti- D serum
- Normal saline
- Glass test tubes (10 × 75 mm )
- Test tube rack
- Pasteur pipette or micro pipette
- Marker
- Container for waste disposal
- Tissue paper
- Specimen-Serum
- Coomb’s control cells: Make pooled ‘O positive blood from at least three different ‘O’ positive blood samples. Wash red cells three times in normal saline so that the cells should be completely free from serum with no free antibodies. Male 5% saline suspension of these cells as follows-Mix 5 drops ( 50µl each) of sedimented RBCs with 2 ml of normal saline. Centrifuge at 1500 RPM for 1 minute and discard the supernatant. Put 4 ml of normal saline into the sedimented RBCs and mix it well. This preparation gives a 5% suspension of RBCs.

The Procedure of Indirect Coomb Test
- Take 3 test tubes and label them as T ( test serum,) PC ( Positive control), and NC (negative control).
- Add two drops of a test serum in tube T.
- Put a drop of Anti-D serum In the tube PC while adding one drop of saline in tube NC.
- Add a drop of 5% saline suspension of the pooled ‘O’ Rho (D) positive cells in each tube.
- Incubate all three tubes for one hour at 37ºC.
- Wash the cells 3 times in normal saline to remove excess serum with no free antibodies.
- Add two drops of anti-human serum (Coomb’s reagent) to each tube. Keep for 5 minutes and then centrifuge at 1,500 RPM for a minute.
- Re-suspend the cells and examine them macroscopically.
- If there is a doubtful finding go with it microscopically.

Result and Interpretation of Indirect Coomb Test

Indirect Coomb Test (ICT) -Negative

Indirect Coomb Test (ICT) -Positive

Clinical Significance of Indirect Coomb Test
This test helps to detect the presence of incomplete free antibodies that may be either Rh antibodies or other antibodies in the patient’s serum in the case of the following :
- To investigate whether an Rh-negative woman married to an Rh-positive husband has developed Anti- Rh antibodies or not.
- Anti-D may be produced in the blood of an Rh-negative person by exposure to D antigen by the following conditions-
- Transfusion of Rh-positive blood
- Pregnancy, if the infant is Rh-positive ( if the father is Rh- positive)
- Abortion of Rh-positive fetus
Keynotes on ICT
- No fasting sample (serum) requires for the Indirect Coomb Test (ICT).
- During the indirect Coomb’S test procedure, adequate washing of the red cells is mandatory otherwise negative results may be obtained.
Further Reading
- https://en.wikipedia.org/wiki/Coombs_test
- https://www.researchgate.net/publication/313146531_The_Direct_Antiglobulin_Test_Indications_Interpretation_and_Pitfalls
- http://www.ijcmaas.com/images/archieve/IJCMAAS_MARCH_2016_VOL10_ISS1_04.pdf
- https://www.nice.org.uk/guidance/cg98/evidence/full-guideline-245411821
- Technical Manual of the American Association of Blood Banks-13th Edition, 1999
- Introduction to Transfusion Medicine –Zarin Bharucha & D.D. Chouhan,1st Edition, 1990
- A Textbook of Medical Laboratory Technology- Darshan P. Godkar Praful B. Godkar