
Introduction
Table of Contents
Corynebacterium diphtheriae is a gram-positive, rod-shaped bacterium that causes diphtheria, a highly contagious and potentially life-threatening respiratory infection. This bacterium was first identified and described by the German physician Edwin Klebs in 1883, and later confirmed by Friedrich Loeffler and Emil von Behring.
The bacterium is named after its characteristic appearance as seen under the microscope. “Coryne” means club-shaped, referring to the distinctive shape of these bacteria. C. diphtheriae is a part of the Corynebacterium genus, which includes several other species, some of which are part of the normal human flora without causing any harm.

Diphtheria is primarily transmitted through respiratory droplets from an infected person. Once the bacterium enters the body, it releases a potent toxin known as diphtheria toxin. This toxin interferes with protein synthesis in human cells, leading to the formation of a thick grayish-white membrane that can develop on the mucous membranes of the throat and other respiratory passages. This membrane can obstruct the airways, causing severe respiratory distress and, in some cases, suffocation.
Historically, diphtheria was a significant cause of mortality, especially in children, before the development of effective vaccines. The introduction of diphtheria vaccination as part of routine childhood immunization programs has significantly reduced the incidence of the disease in many parts of the world.
Treatment of diphtheria involves the administration of diphtheria antitoxin to neutralize the effects of the toxin and antibiotics to eradicate the bacterium. Prompt medical attention is crucial to improve the chances of recovery and reduce complications.
As with any infectious disease, prevention is key. Vaccination remains the most effective way to protect against diphtheria. The diphtheria toxoid vaccine, often combined with tetanus and pertussis vaccines, is widely used and recommended as part of routine immunization schedules. Regular booster shots are necessary to maintain immunity throughout life.
Morphology
Corynebacterium diphtheriae is a gram-positive bacterium with a distinct morphological appearance. Under the microscope, it appears as a slender, rod-shaped cell with rounded ends. The individual cells are typically arranged in a characteristic manner, giving rise to specific arrangements or patterns. The key morphological features of C. diphtheriae are as follows:
- Shape: The bacterium is rod-shaped, often referred to as bacilli. These rods are straight or slightly curved and can vary in length from 1 to 8 micrometers.
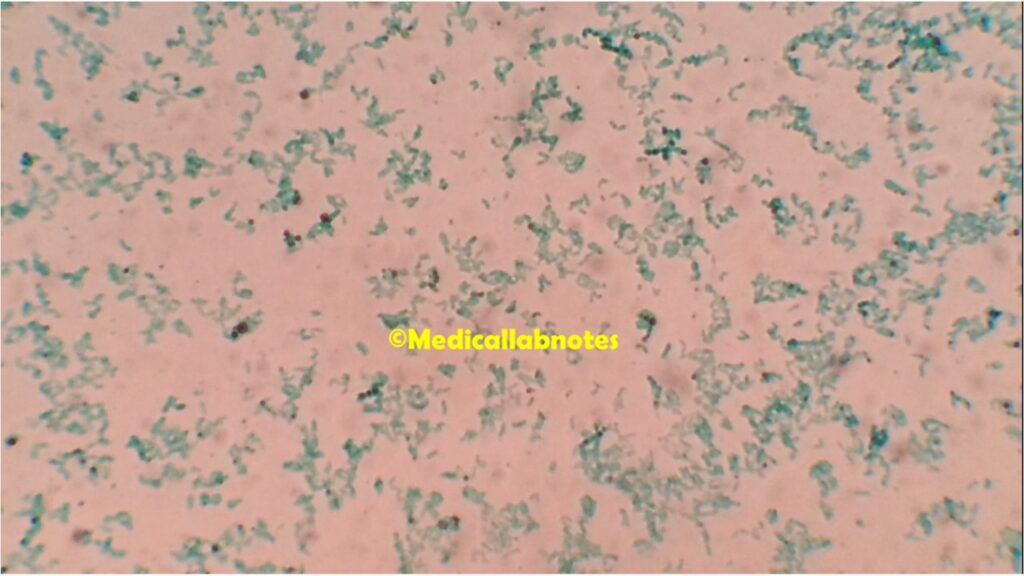
- Arrangement: Corynebacterium diphtheriae cells can arrange themselves in various patterns, with the most common being palisades or “Chinese letters” arrangement. In this pattern, the cells align parallel to each other, resembling a row of fence posts or Chinese characters.
- Palisades: In the palisades arrangement, the cells align closely and side-by-side, resulting in a characteristic appearance when stained and observed under the microscope.
- Pleomorphic: Corynebacterium diphtheriae can exhibit some degree of pleomorphism, meaning they may appear in different shapes or sizes within a population.
- Gram staining: The bacterium is gram-positive, which means it retains the violet stain in the Gram staining procedure. This is due to the presence of a thick peptidoglycan layer in the cell wall.
- Metachromatic granules: When stained with certain dyes, Corynebacterium diphtheriae may exhibit metachromatic granules, which appear as red or blue inclusions within the cells. These granules are composed of polyphosphate, and their presence is characteristic of the species.
Pathogenicity
Corynebacterium diphtheriae is a highly pathogenic bacterium responsible for causing diphtheria, a potentially life-threatening infectious disease. The pathogenicity of C. diphtheriae is mainly attributed to its ability to produce a powerful exotoxin known as the diphtheria toxin. This toxin is one of the most potent bacterial toxins and plays a central role in the development of diphtheria symptoms.
Pathogenesis of Corynebacterium diphtheriae:
- Transmission: The bacterium is primarily transmitted through respiratory droplets when an infected person coughs or sneezes, or by direct contact with infected individuals or carriers. It can also spread through contact with items contaminated by respiratory secretions, such as shared utensils or toys.
- Adhesion and colonization: After inhalation or entry through mucosal surfaces, C. diphtheriae adheres to and colonizes the epithelial cells lining the upper respiratory tract, especially the throat and tonsils.
- Production of Diphtheria Toxin: The critical virulence factor of C. diphtheriae is the diphtheria toxin. It is encoded by a gene present on a bacteriophage (a virus that infects bacteria) that can integrate into the bacterial genome. The toxin is produced by lysogenic (toxin-producing) strains of C. diphtheriae. The bacteriophage carries the genetic information for toxin production and is essential for the bacterium to become toxigenic.
- Diphtheria Toxin Mechanism of Action: The diphtheria toxin functions as an A-B toxin, with an enzymatically active “A” subunit and a cell-binding “B” subunit. The “B” subunit binds to specific receptors on the surface of host cells, facilitating the entry of the “A” subunit into the cells. Once inside the host cell, the “A” subunit inactivates elongation factor 2 (EF-2), a protein involved in protein synthesis, leading to cell death. The inhibition of protein synthesis results in the formation of a characteristic pseudomembrane in the throat, composed of dead tissue, fibrin, and bacterial cells.
- Pseudomembrane Formation: The diphtheria toxin damages the host’s respiratory epithelial cells, leading to the formation of a thick grayish-white pseudomembrane in the throat and other respiratory passages. This membrane can obstruct the airways, causing severe respiratory distress and potentially leading to suffocation if not treated promptly.
- Systemic Effects: In addition to the local effects in the respiratory tract, the diphtheria toxin can enter the bloodstream, causing systemic complications. It can lead to damage to organs, nerves, and the heart. The toxin can also cause myocarditis, a condition that affects the heart muscle and can lead to heart failure.
Lab Diagnosis
The laboratory diagnosis of Corynebacterium diphtheriae involves various techniques to identify and confirm the presence of the bacterium and its toxin. Prompt and accurate diagnosis is crucial for initiating appropriate treatment and implementing control measures to prevent further spread. The following are some common methods used for the laboratory diagnosis of C. diphtheriae:
- Clinical Examination: The first step in the diagnosis is a thorough clinical examination of the patient, paying attention to symptoms such as a sore throat, difficulty swallowing, and the presence of a grayish-white membrane in the throat or tonsils.
- Collection of Specimens: To isolate C. diphtheriae, swab samples are taken from the throat or any other suspected site of infection, such as the skin or wounds.
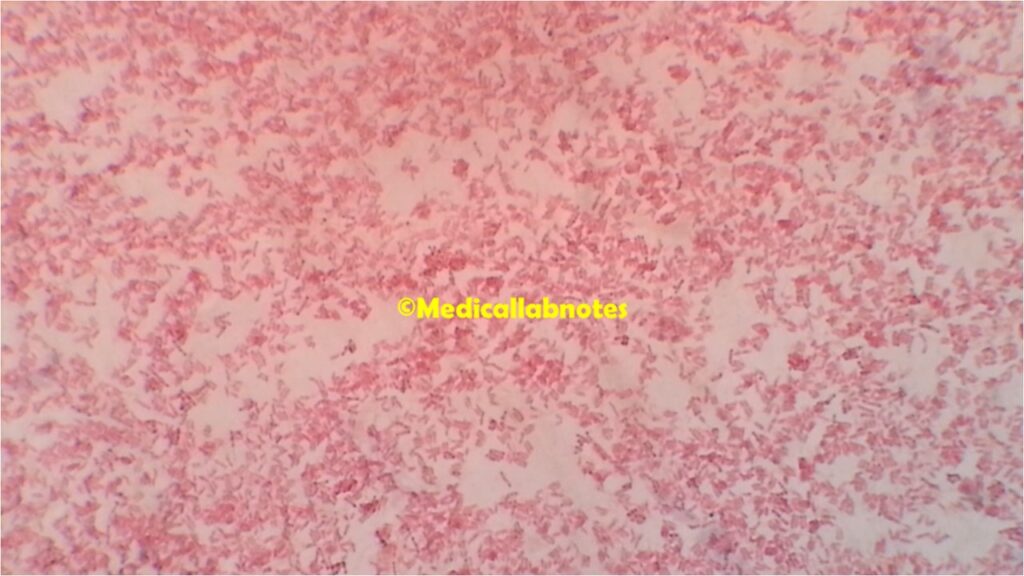
- Gram Stain: The collected samples are subjected to a Gram stain to visualize the characteristic gram-positive, rod-shaped bacteria. C. diphtheriae appears as Gram-positive rods, often arranged in palisades or Chinese letter-like formations.
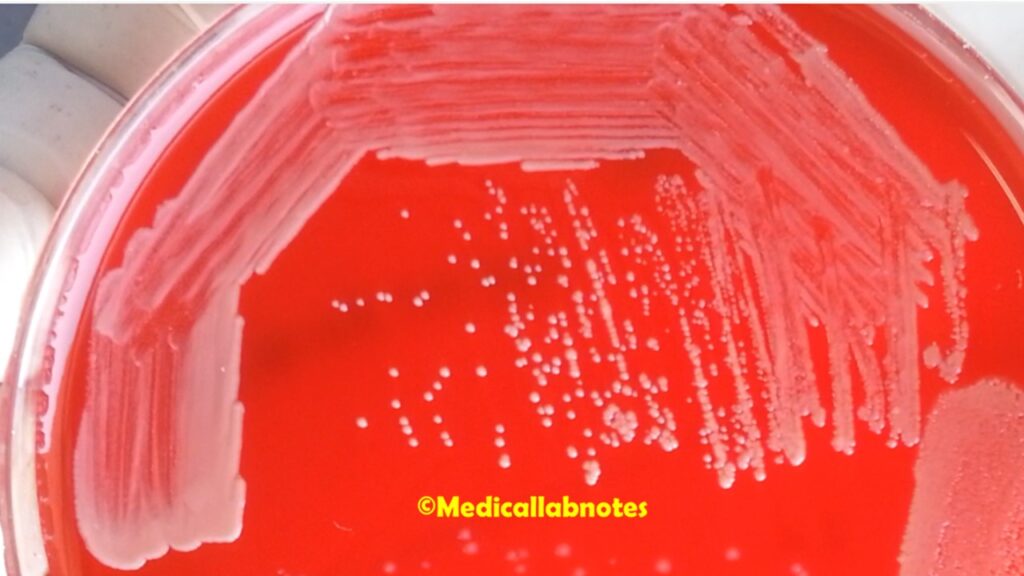
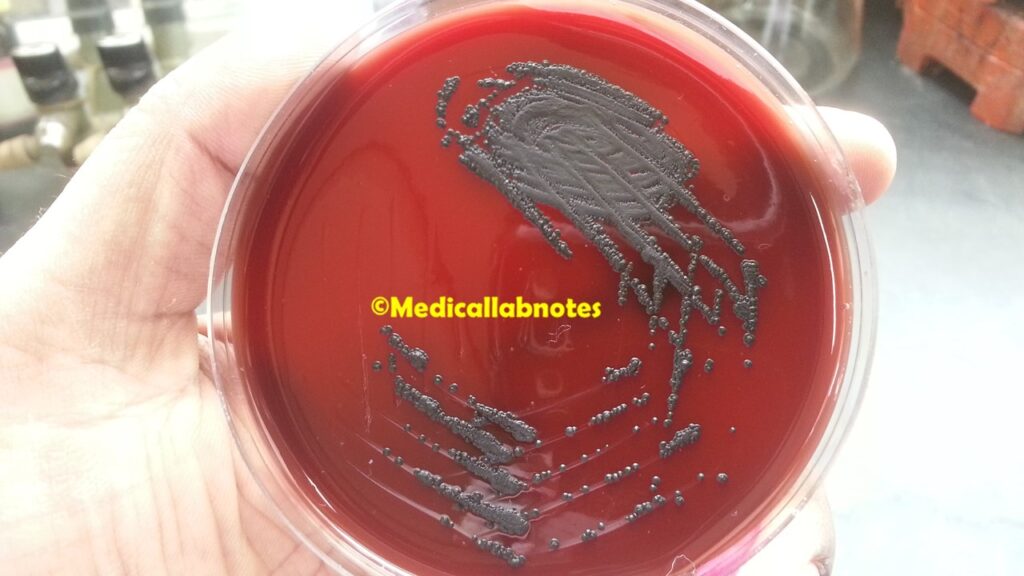
- Culture: The primary method for diagnosing diphtheria is by isolating C. diphtheriae in culture. The swab samples are inoculated onto specific culture media like Loeffler’s or Tinsdale agar, which are selective for Corynebacterium species. The bacteria grow on the agar, forming characteristic colonies.
- Biochemical Tests: Biochemical tests are performed to confirm the identity of the isolated colonies as C. diphtheriae. These tests can include catalase, urease, and fermentation tests, among others.
- Elek Test: To determine the toxigenicity of the isolated C. diphtheriae strains, the Elek test is used. This test involves streaking a C. diphtheriae culture on a special agar plate and placing filter paper strips soaked with diphtheria antitoxin adjacent to the streaks. If the bacterium produces the diphtheria toxin, a visible precipitin line will form between the bacterial streaks and the antitoxin-soaked paper strips.
- Polymerase Chain Reaction (PCR): PCR can be used to detect the presence of the diphtheria toxin gene in isolated bacterial colonies, providing a rapid and specific identification of toxigenic strains.

It is essential to follow strict biosafety protocols when working with suspected C. diphtheriae isolates due to its pathogenicity. All suspected isolates should be handled in a biosafety level 2 (BSL-2) laboratory to prevent any potential transmission.

In addition to laboratory testing, clinical diagnosis, and vaccination history are essential components in the overall diagnosis of diphtheria. If diphtheria is suspected, appropriate public health authorities should be notified promptly to initiate appropriate control measures and contact tracing to prevent further transmission.
Treatment
The treatment of Corynebacterium diphtheriae infection, commonly known as diphtheria, involves a combination of antitoxin therapy, antibiotic treatment, and supportive care. Prompt initiation of treatment is crucial to prevent complications and improve patient outcomes. Treatment measures include:

- Diphtheria Antitoxin (DAT): Diphtheria antitoxin is the cornerstone of treatment for diphtheria. The antitoxin is derived from the blood of horses immunized with diphtheria toxin. It contains antibodies that neutralize the circulating diphtheria toxin in the patient’s body. The DAT is administered intravenously and should be given as soon as diphtheria is suspected, even before the definitive laboratory confirmation. Early administration of antitoxin is essential to prevent the progression of the disease and reduce the severity of symptoms.
- Antibiotic Therapy: Concurrently with the administration of diphtheria antitoxin, antibiotics are prescribed to eradicate the bacteria from the patient’s system. Penicillin or erythromycin are commonly used antibiotics for the treatment of diphtheria. In cases of penicillin allergy, alternative antibiotics like clindamycin or azithromycin may be used.
- Supportive Care: Patients with diphtheria may require supportive care to manage complications and symptoms. This includes measures to maintain airway patency, oxygen therapy, hydration, and nutrition support.
- Isolation and Infection Control: Patients diagnosed with diphtheria should be isolated to prevent the spread of the bacterium to others. Infection control measures, including strict hand hygiene and respiratory precautions, are essential in healthcare settings and for close contacts of the infected individual.
- Immunization: Ensuring complete and timely immunization against diphtheria is critical to preventing the disease. Routine childhood immunization schedules include the diphtheria toxoid vaccine, often combined with tetanus and pertussis vaccines (DTaP or Tdap). Booster doses of the vaccine are necessary throughout life to maintain immunity.
- Post-Exposure Prophylaxis: Individuals who have been in close contact with a confirmed diphtheria case may be offered post-exposure prophylaxis with diphtheria toxoid vaccine or diphtheria antitoxin, depending on their vaccination status and risk of infection.
It is essential to note that diphtheria is a notifiable disease in many countries, and healthcare providers are required to report all suspected and confirmed cases to the public health authorities. Early diagnosis, immediate treatment, and public health measures are critical to preventing further transmission and outbreaks of diphtheria.
Prevention
The prevention of Corynebacterium diphtheriae infection, commonly known as diphtheria, primarily relies on vaccination and public health measures. Here are the key strategies for preventing diphtheria:

- Vaccination: Routine vaccination with the diphtheria toxoid vaccine is the most effective way to prevent diphtheria. The vaccine is usually administered in combination with tetanus and pertussis vaccines (DTaP or Tdap). In some regions, it may be given as part of a pentavalent vaccine (DTaP-IPV-Hib) that also includes protection against Haemophilus influenzae type b and inactivated poliovirus.
- Childhood Immunization: Diphtheria vaccination is typically included in the childhood immunization schedule. It is administered as a series of doses starting at 2 months of age, with booster shots at regular intervals throughout childhood.
- Booster Doses: To maintain immunity, booster doses of the diphtheria toxoid vaccine are recommended during adolescence and adulthood. In some countries, the Tdap vaccine is given to adolescents as a booster to provide protection against diphtheria, tetanus, and pertussis.
- Timely Vaccination: It is crucial to adhere to the recommended vaccination schedule to ensure that individuals receive the necessary doses at appropriate intervals. Delaying or skipping vaccinations can leave individuals susceptible to diphtheria and other preventable diseases.
- Post-Exposure Prophylaxis: Individuals who have been in close contact with a confirmed diphtheria case, especially those who are not fully vaccinated, may receive post-exposure prophylaxis. This may include a booster dose of the diphtheria toxoid vaccine or administration of diphtheria antitoxin, depending on the individual’s vaccination status and risk of infection.
- Public Health Measures: In addition to vaccination, public health measures play a crucial role in preventing the spread of diphtheria:
- Surveillance and Reporting: Timely surveillance and reporting of suspected and confirmed cases are essential for early detection and control of outbreaks.
- Isolation and Infection Control: Patients with suspected or confirmed diphtheria should be isolated to prevent transmission to others. Healthcare facilities should implement appropriate infection control measures to limit the spread of the bacterium.
- Contact Tracing: Identifying and monitoring individuals who have been in close contact with confirmed cases can help prevent further transmission.
- Health Education: Public health authorities should educate the public about the importance of vaccination, recognize the signs and symptoms of diphtheria, and promote hygiene practices to reduce the risk of transmission.

Keynotes
Corynebacterium diphtheriae is a gram-positive bacterium responsible for causing diphtheria, a highly contagious respiratory infection. Here are some keynotes on C. diphtheriae:

- Morphology: C. diphtheriae is a rod-shaped bacterium with rounded ends. It appears as Gram-positive rods under the microscope and often forms palisades or Chinese letter-like arrangements.
- Transmission: The bacterium spreads through respiratory droplets from infected individuals. It can also be transmitted through contact with items contaminated by respiratory secretions.
- Diphtheria Toxin: The critical virulence factor of C. diphtheriae is the diphtheria toxin, produced by lysogenic strains carrying a bacteriophage encoding the toxin gene.
- Diphtheria Disease: Diphtheria presents with symptoms such as a sore throat, fever, difficulty swallowing, and the formation of a grayish-white pseudomembrane in the throat and tonsils. Severe cases can lead to respiratory distress and systemic complications.
- Prevention: Vaccination with diphtheria toxoid vaccine is the primary method of prevention. Booster shots throughout life help maintain immunity.
- Laboratory Diagnosis: Diagnosis involves clinical examination, Gram stain, culture on selective media, biochemical tests, and the Elek test to detect toxin production.
- Treatment: Treatment includes administration of diphtheria antitoxin to neutralize the toxin and antibiotics (penicillin or erythromycin) to eradicate the bacterium.
- Public Health Measures: Isolation of infected individuals, contact tracing, and strict infection control measures are essential to prevent the spread of diphtheria.
- Post-Exposure Prophylaxis: Close contacts may receive post-exposure prophylaxis with vaccination or antitoxin, depending on their vaccination status and risk of infection.
- Global Impact: Routine vaccination and public health efforts have significantly reduced the incidence of diphtheria worldwide, but the disease remains a concern in areas with low vaccination rates or during outbreaks.

Further Readings
- CDC – Diphtheria: Information about diphtheria, its symptoms, transmission, prevention, and treatment from the Centers for Disease Control and Prevention (CDC). Website: https://www.cdc.gov/diphtheria/index.html
- World Health Organization (WHO) – Diphtheria: Information on diphtheria from the WHO, including global data, vaccination strategies, and outbreak response. Website: https://www.who.int/health-topics/diphtheria
- Medical Microbiology, 8th Edition, Chapter 16 – Corynebacterium, Arcanobacterium, and Rhodococcus: A comprehensive textbook chapter covering the microbiology, pathogenesis, and clinical aspects of Corynebacterium species, including C. diphtheriae. Authors: Samuel Baron. Book: https://www.ncbi.nlm.nih.gov/books/NBK7617/
- Diphtheria Toxin and Its Mode of Action: A review article that delves into the molecular mechanism of diphtheria toxin, its structure, and its interactions with host cells. Authors: Vikas Navratna, Rishabh Singh, and Jyoti Kumari. Journal: Toxins. 2020, 12(11), 747. DOI: 10.3390/toxins12110747
- Diphtheria: Forgotten but Not Gone: An article discussing the resurgence of diphtheria in some regions and the importance of maintaining high vaccination coverage. Authors: Scott Olesen and Daniel O’Connor. Journal: The Pediatric Infectious Disease Journal. 2017, 36(6), 590-592. DOI: 10.1097/INF.0000000000001531
- The Return of Epidemic Diphtheria in a European Country: Challenges for Diagnosis and Control: A case report describing a diphtheria outbreak in a European country and the challenges faced in diagnosis and control. Authors: K. L. White, A. A. Pombubpa, J. M. Sohail, et al. Journal: Journal of Clinical Microbiology. 2019, 57(6), e00122-19. DOI: 10.1128/JCM.00122-19
- Molecular Typing and Characterization of Corynebacterium diphtheriae and Corynebacterium ulcerans Strains Isolated in Italy: A research article exploring the molecular characterization of C. diphtheriae and C. ulcerans strains in Italy. Authors: E. Camilli, R. D’Ambrosio, M. L. D. Cunha, et al. Journal: New Microbes and New Infections. 2016, 9, 47-54. DOI: 10.1016/j.nmni.2015.12.009