
Introduction
Table of Contents
Fonsecaea is a genus of fungi commonly associated with human and animal infections. It belongs to the class Eurotiomycetes and the order Chaetothyriales. The most clinically relevant species within this genus is Fonsecaea pedrosoi, which is known to cause chromoblastomycosis, a chronic and localized fungal infection of the skin and subcutaneous tissues.
Chromoblastomycosis is primarily a disease of tropical and subtropical regions, and it is typically contracted through traumatic inoculation of fungal spores into the skin. Once the spores are introduced into the body, they can establish a chronic infection that presents as nodular lesions, warty growths, and discolored skin patches. These lesions often resemble cauliflower-like structures and can be quite difficult to treat.
Fonsecaea species, including Fonsecaea pedrosoi, are dematiaceous fungi, meaning they have darkly pigmented cell walls due to the presence of melanin. This pigmentation helps the fungi protect themselves from environmental stressors and immune responses.
Diagnosis of chromoblastomycosis caused by Fonsecaea species usually involves a combination of clinical evaluation, microscopic examination of tissue samples, and fungal culture. Treatment can be challenging due to the chronic nature of the infection and the resistance of the fungi to many antifungal drugs. Therapeutic options often include a combination of surgical excision, antifungal medications, and physical therapies.
Morphology
The morphology of Fonsecaea species, particularly Fonsecaea pedrosoi, is characterized by certain distinctive features that help identify these fungi. Fonsecaea species are dematiaceous fungi, which means they have pigmented cell walls due to the presence of melanin. Here are some key aspects of the morphology of Fonsecaea:
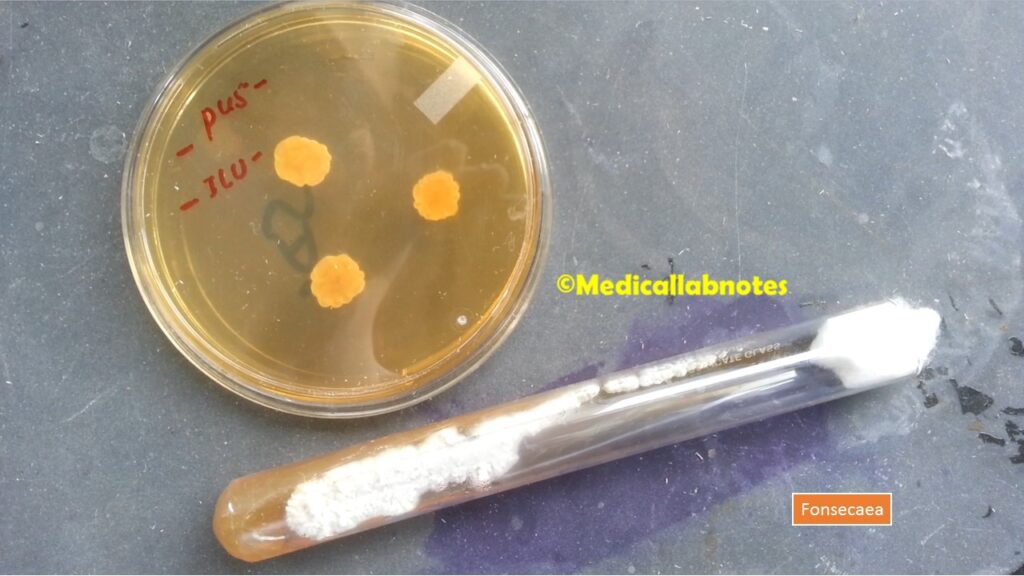
- Colonial Characteristics: They typically form colonies on culture media that are darkly pigmented, ranging from brown to black. The colonies can have a velvety or woolly texture and often exhibit slow growth.
- Hyphal Structure: The hyphae (filamentous structures) of Fonsecaea species are septate, meaning they are divided into segments by cross-walls called septa. These septa are typically darkly pigmented due to the presence of melanin.
- Conidia: Conidia are asexual spores produced by the fungi for reproduction. In Fonsecaea species, conidia are typically borne on specialized structures called conidiophores. The conidia are oval to ellipsoidal in shape and are darkly pigmented, often appearing brown or black. The conidia can vary in size but are generally small.
- Sclerotic Cells: One of the distinguishing features of Fonsecaea pedrosoi is the formation of sclerotic cells, also known as muriform cells or “Medlar bodies.” These are thick-walled, multicellular structures that have a characteristic brick-like appearance. Sclerotic cells are the hallmark of chromoblastomycosis and are found within the skin lesions of infected individuals.
- Dimorphic Nature: F. pedrosoi is considered a dimorphic fungus, meaning it can exist in two different growth forms depending on environmental conditions. In its mold form, it grows as hyphae and produces conidia. In its yeast form, it transforms into round-to-oval cells that are typically found in tissues during the infection.
- Microscopic Examination: When examined under a microscope, the presence of darkly pigmented hyphae, septa, conidiophores, and conidia are key features for identifying Fonsecaea species.
Pathogenicity
Fonsecaea species, particularly F. pedrosoi, are considered opportunistic pathogens that can cause a specific fungal infection known as chromoblastomycosis. Here’s an overview of the pathogenicity of Fonsecaea:
Chromoblastomycosis: Chromoblastomycosis is a chronic fungal infection primarily caused by F. pedrosoi, among other related fungi. This infection is characterized by the formation of nodular, warty, and discolored lesions on the skin and subcutaneous tissues. It is typically acquired through traumatic implantation of fungal spores into the skin, often in tropical and subtropical regions.
The pathogenesis of chromoblastomycosis involves several stages:
- Initial Inoculation: The fungal spores, which are often present in soil and organic matter, are introduced into the skin through minor injuries, cuts, or abrasions.
- Formation of Sclerotic Cells: Once inside the body, the fungus undergoes a transformation. The yeast-like cells of Fonsecaea transform into thick-walled, multicellular structures known as sclerotic cells or “Medlar bodies.” These cells have a distinctive appearance and are characteristic of the disease.
- Chronic Infection: The sclerotic cells are not readily recognized by the immune system, allowing the infection to persist. Over time, they provoke an inflammatory response that leads to the development of the characteristic nodular and verrucous skin lesions.
- Secondary Dissemination: In some cases, the infection may progress and lead to secondary dissemination, spreading to deeper tissues or affecting nearby lymph nodes.
The exact mechanisms underlying the ability of Fonsecaea species to cause chromoblastomycosis are not fully understood. However, the pigmented nature of these fungi, attributed to melanin production, is thought to play a role in their ability to evade host immune responses. Melanin is known to have immunomodulatory properties and could contribute to fungal survival within the host.
Lab Diagnosis
The laboratory diagnosis of infections caused by Fonsecaea species, particularly chromoblastomycosis, involves a combination of clinical evaluation, microscopy, culture, and molecular techniques. Here’s an overview of the diagnostic methods used:

- Clinical Evaluation: A thorough clinical assessment is essential, as the characteristic nodular, verrucous, or cauliflower-like skin lesions are often indicative of chromoblastomycosis. The clinical presentation, history of exposure to risk factors (such as outdoor activities in tropical regions), and progression of the lesions provide important clues for diagnosis.
- Microscopy: Microscopic examination of tissue samples or exudates from skin lesions can reveal the presence of fungal elements. Key features to look for include:
- Sclerotic Cells: The presence of characteristic brick-like sclerotic cells within the tissue samples is a hallmark of chromoblastomycosis caused by Fonsecaea species. These cells can be observed in skin scrapings or biopsy specimens.
- Hyphal Structures: Examination of the tissue samples may reveal septate hyphae, conidiophores, and conidia, which can help identify the specific fungal genus.
- Fungal Culture: Culturing the fungus from clinical specimens is an important step for definitive identification. However, Fonsecaea species can be slow-growing and challenging to culture. The following steps are typically taken:
- Sabouraud’s Agar: Clinical specimens, such as skin scrapings or biopsy samples, are inoculated onto Sabouraud’s agar, a standard fungal culture medium.
- Dark Conditions: Cultures are incubated in the dark to promote the growth of pigmented fungi like Fonsecaea.
- Slow Growth: They usually exhibit slow growth and may take several weeks to months to produce visible colonies.
- Molecular Techniques: Molecular methods, such as polymerase chain reaction (PCR) and DNA sequencing, can provide accurate and rapid species identification. These techniques are particularly useful when the clinical presentation is atypical or when traditional methods yield inconclusive results.
- PCR: Specific primers can be designed to amplify fungal DNA, allowing for the detection of Fonsecaea species.
- DNA Sequencing: Sequencing the amplified DNA fragments can provide precise species identification based on genetic markers.
- Histopathology: In cases of deep or invasive infections, histopathological examination of biopsy samples can provide insights into tissue invasion, inflammation, and fungal morphology.
Treatment
The treatment of Fonsecaea infections, particularly chromoblastomycosis caused by F. pedrosoi, can be challenging due to the chronic nature of the infection and the resistance of the fungus to many antifungal medications. Treatment approaches often involve a combination of surgical procedures, antifungal medications, and physical therapies. The choice of treatment depends on the severity of the infection, the extent of tissue involvement, and the overall health of the patient.
Here are the main treatment strategies used for Fonsecaea infections:
- Surgical Excision: Surgical removal of the infected tissue can be effective in reducing the fungal burden and promoting healing. However, complete removal of the lesions can be difficult, especially when the infection has spread to deeper tissues. Surgery is often combined with other treatment modalities.
- Antifungal Medications: Various antifungal drugs can be used to treat Fonsecaea infections, but response rates can vary and complete cure is not always achieved. Some of the commonly used antifungal agents include:
- Itraconazole: This azole antifungal is often considered the first-line treatment. It is taken orally and has been shown to have some effectiveness in reducing lesion size and controlling the infection.
- Terbinafine: Another oral antifungal, terbinafine, has shown activity against Fonsecaea species. It is sometimes used in combination with itraconazole.
- Posaconazole: Posaconazole is an extended-spectrum azole antifungal that may be considered when other treatments fail or in cases of resistance.
- Amphotericin B: In severe cases or cases unresponsive to other therapies, intravenous amphotericin B may be considered. However, its use is often limited due to potential side effects.
- Physical Therapies: Physical therapies can be used as adjunctive treatments to enhance the effectiveness of antifungal drugs:
- Heat Therapy (Thermotherapy): Localized heat application to the lesions can help weaken the fungal cells and enhance the penetration of antifungal agents.
- Cryotherapy (Freezing): Freezing the lesions with liquid nitrogen can destroy the fungal cells and promote healing.
- Laser Therapy: Laser treatment can be used to target and destroy the fungal cells, often in combination with antifungal medications.
It’s important to note that the duration of treatment can be prolonged, often lasting several months to years, and successful outcomes are not always guaranteed. Regular monitoring of the patient’s progress and response to treatment is essential to adjust the therapeutic approach as needed.
Prevention
Preventing infections caused by Fonsecaea species, particularly chromoblastomycosis, involves taking precautions to minimize exposure to fungal spores in the environment. While complete avoidance of exposure may not always be feasible, especially for individuals living in endemic areas, there are several steps that can be taken to reduce the risk of infection:
- Protective Clothing: When engaging in outdoor activities in areas where Fonsecaea infections are known to occur, consider wearing long-sleeved shirts, long pants, and closed-toe shoes to minimize direct contact with soil and vegetation.
- Footwear: Proper footwear can help protect your feet from accidental injuries that could lead to fungal spore entry. Avoid walking barefoot in environments where fungal exposure is a concern.
- Wound Care: Promptly clean and properly care for any cuts, scrapes, or wounds to minimize the risk of fungal spores entering the skin.
- Avoid Trauma: Take precautions to avoid traumatic injuries, as these can serve as entry points for fungal spores. Be cautious when working with tools, equipment, or materials that could cause cuts or abrasions.
- Hygiene: Good personal hygiene can help prevent fungal infections. Keep your skin clean and dry, especially in areas prone to sweating.
- Avoid Contaminated Materials: Avoid contact with materials that may be contaminated with fungal spores, such as decomposing plant matter, soil, and stagnant water.
- Occupational Safety: Individuals working in agricultural or outdoor settings should be aware of the potential risks of fungal exposure and follow occupational safety guidelines.
- Education: Individuals living in or traveling to endemic regions should be educated about the signs, symptoms, and risk factors associated with chromoblastomycosis. Early recognition and treatment can help prevent the progression of the infection.
- Early Treatment: If you notice any suspicious skin lesions or changes, seek medical attention promptly. Early diagnosis and treatment can prevent the infection from becoming chronic and more difficult to manage.
- Immunocompromised Individuals: Individuals with weakened immune systems, such as those with HIV/AIDS or undergoing immunosuppressive treatments, should take extra precautions to avoid exposure to fungal pathogens.
Keynotes
Here are some key points to remember about Fonsecaea:
- Genus and Species: It is a genus of fungi, and F. pedrosoi is the most clinically significant species within this genus.
- Pathogenicity: Fonsecaea species, especially F. pedrosoi, are responsible for causing chromoblastomycosis, a chronic fungal infection primarily affecting the skin and subcutaneous tissues.
- Chromoblastomycosis: Chromoblastomycosis is characterized by the formation of nodular, warty, and discolored skin lesions. It is often contracted through traumatic implantation of fungal spores into the skin.
- Clinical Presentation: The infection presents as cauliflower-like growths with nodules, often resembling warts. These lesions can be difficult to treat due to their chronic nature.
- Sclerotic Cells: F. pedrosoi forms characteristic brick-like sclerotic cells or “Medlar bodies” within the skin lesions, which are a diagnostic feature of chromoblastomycosis.
- Dematiaceous Fungi: They are dematiaceous fungi, meaning they have darkly pigmented cell walls due to the presence of melanin. This pigmentation helps them survive in diverse environments.
- Lab Diagnosis: Diagnosis involves clinical assessment, microscopic examination of tissue samples (looking for sclerotic cells and hyphal structures), fungal culture, and molecular techniques like PCR and DNA sequencing.
- Treatment: Treating Fonsecaea infections involves a combination of surgical excision, antifungal medications (e.g., itraconazole, terbinafine), and physical therapies (thermotherapy, cryotherapy). Treatment can be prolonged and challenging.
- Prevention: Preventive measures include wearing protective clothing, avoiding trauma and injuries, maintaining good hygiene, and seeking early medical attention for suspicious skin changes.
- Geographical Distribution: Chromoblastomycosis caused by Fonsecaea species is more common in tropical and subtropical regions, where exposure to fungal spores is higher.
- Immunocompromised Individuals: Individuals with weakened immune systems are more susceptible to Fonsecaea infections, and infections in these individuals can be more severe and difficult to manage.
- Research: Ongoing research aims to improve the understanding of the epidemiology, pathogenesis, and treatment of Fonsecaea infections to enhance patient outcomes.
Further Readings
- Medical Journals and Research Articles:
- Look up articles on Fonsecaea and chromoblastomycosis in medical journals such as “Journal of Clinical Microbiology,” “Mycopathologia,” “Journal of Dermatological Science,” and “Medical Mycology.”
- Textbooks and Reference Books:
- “Clinical Mycology” by Elias J. Anaissie, Michael R. McGinnis, and Michael A. Pfaller.
- “Topley & Wilson’s Microbiology and Microbial Infections” edited by Stefan H. E. Kaufmann, Barry I. L. Cohen, and Michael J. Blaser.
- “Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases” edited by John E. Bennett, Raphael Dolin, and Martin J. Blaser.
- Online Resources:
- The Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) websites may have information on fungal infections, including rare ones like Fonsecaea-related infections.
- The Mycology Online website by the University of Adelaide provides valuable information on various fungal infections, including chromoblastomycosis and related fungi.
- Dermatology and Infectious Disease Organizations:
- The American Academy of Dermatology (AAD) and the Infectious Diseases Society of America (IDSA) might have clinical guidelines and resources on fungal infections.
- Scientific Databases:
- PubMed, Google Scholar, and other academic databases can help you find recent research articles, case studies, and reviews related to Fonsecaea and chromoblastomycosis.
- Consulting Specialists:
- If you’re a medical professional or student, consider reaching out to dermatologists, infectious disease specialists, or medical mycologists for guidance and recommended readings.
Hey There. I discovered your weblog the use of msn. This is a really neatly written article. I’ll be sure to bookmark it and come back to read extra of your useful information. Thanks for the post. I’ll certainly return.