
Introduction
Table of Contents
Mycobacterium leprae is the bacterium responsible for causing leprosy, also known as Hansen’s disease. It is an ancient disease that has afflicted humans for thousands of years, and it continues to be a significant public health concern in some parts of the world.
M. leprae is a slow-growing, acid-fast, intracellular bacterium. It primarily infects peripheral nerves, the skin, and other mucous membranes. The bacterium’s unique properties contribute to the chronic nature of leprosy and its ability to remain undetected in the human body for extended periods, leading to long incubation periods that can range from months to several years.
Leprosy primarily affects the skin and peripheral nerves, leading to various symptoms such as skin lesions, disfigurement, and nerve damage. The disease manifests in different forms, with the two most common types being tuberculoid leprosy and lepromatous leprosy, representing the poles of the disease spectrum. The tuberculoid form is milder and exhibits a cell-mediated immune response, while the lepromatous form is more severe and characterized by a weaker immune response.
Leprosy is primarily transmitted through respiratory droplets when an infected person coughs or sneezes. Despite its chronic nature, leprosy is not highly contagious, and the majority of people are naturally immune to the disease. Early diagnosis and timely treatment with multi-drug therapy (MDT) are essential to prevent complications and disability associated with leprosy.
Although significant progress has been made in controlling leprosy through various global initiatives, it remains a concern in certain regions, particularly in countries with limited healthcare resources and poor living conditions. Efforts to combat leprosy focus on early detection, raising awareness, reducing stigma, and providing accessible and effective treatment to affected individuals.
Morphology
The morphology of Mycobacterium leprae is distinctive and plays a significant role in its identification and classification. As an acid-fast bacterium, it shares certain characteristics with other members of the Mycobacterium genus, but it also possesses some unique features specific to leprosy-causing bacteria.

- Shape: M. leprae is a rod-shaped bacterium, appearing as slender and elongated under a microscope.
- Size: It is an exceptionally small bacterium, with a length of about 1-8 micrometers and a width of 0.2-0.5 micrometers. Its tiny size is one of the reasons why it can invade and inhabit human peripheral nerves and other tissues.
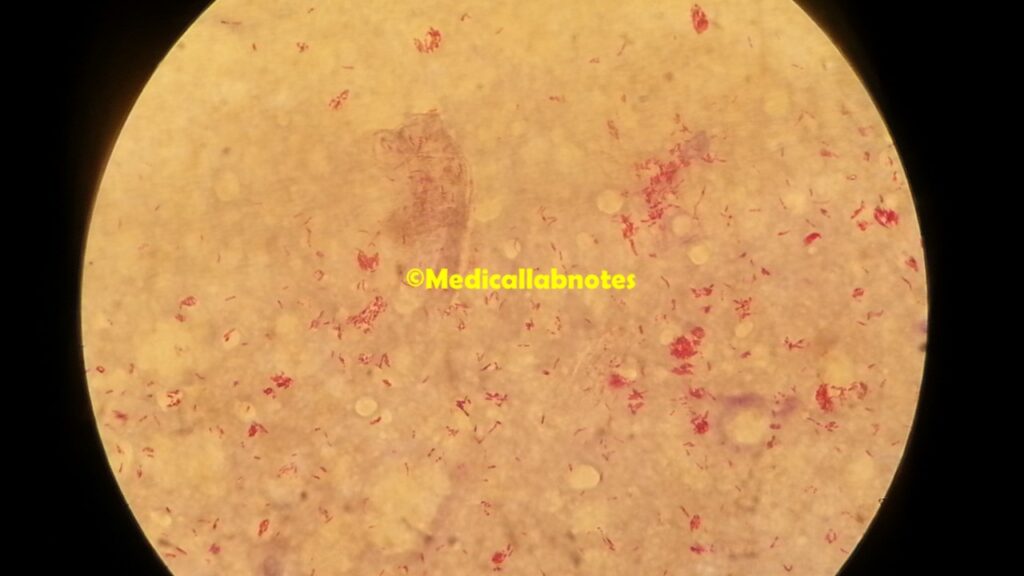
- Acid-fast staining: One of the most notable features of Mycobacterium leprae is its ability to retain certain dyes, even after washing with acidic solutions. This property is referred to as acid-fastness and is due to the high lipid content in its cell wall. The classic staining method used for Mycobacterium leprae is the Ziehl-Neelsen stain or the Kinyoun stain, which imparts a red color to the bacteria.
- No Gram staining: Mycobacterium leprae is non-Gram staining, meaning it does not retain the crystal violet dye used in the Gram staining technique for bacterial classification. This is because its cell wall composition is different from both Gram-positive and Gram-negative bacteria.
- Obligate intracellular pathogen: It is an obligate intracellular pathogen, which means it can only replicate within the cells of the host organism. In the case of leprosy, it primarily infects macrophages, Schwann cells, and endothelial cells of the skin and peripheral nerves.
- Slow growth: The bacterium has an extremely slow growth rate, with a generation time of about 14 days. This slow growth contributes to the long incubation period and chronic nature of leprosy.
It’s important to note that due to its unique characteristics, Mycobacterium leprae cannot be cultured in artificial laboratory media, making it challenging to study and limiting the understanding of its biology. Diagnosis of leprosy is typically achieved through clinical and histopathological examination of skin biopsies, molecular methods (polymerase chain reaction), and slit-skin smears to detect the bacilli in affected tissues.
Pathogenicity
The pathogenicity of Mycobacterium leprae is the ability of this bacterium to cause disease, leading to the clinical manifestations of leprosy or Hansen’s disease. M. leprae is an obligate intracellular pathogen, meaning it can only survive and multiply within the cells of the host organism. This unique feature plays a significant role in the pathogenesis of leprosy.
Key aspects of the pathogenicity of Mycobacterium leprae are as follows:
- Entry and infection: It primarily enters the human body through the respiratory route when an infected person coughs or sneezes, releasing bacteria-containing droplets. These droplets may be inhaled by individuals in close contact, leading to infection. However, it is essential to note that the majority of people have a natural immunity to leprosy, and not all exposed individuals will develop the disease.
- Invasion and intracellular survival: Once Mycobacterium leprae gains entry into the body, it invades the host’s immune cells, particularly macrophages, as well as Schwann cells (nerves) and endothelial cells in the skin and peripheral nerves. The bacterium’s unique cell wall composition, rich in lipids like mycolic acid, helps it resist destruction by the host’s immune system. It also inhibits the normal maturation of the phagolysosome, a cellular compartment involved in the destruction of pathogens, allowing the bacterium to survive and multiply within the host cells.
- Immune response: The host’s immune response to M. leprae plays a crucial role in determining the clinical presentation of leprosy. The spectrum of the disease ranges from a tuberculoid form, characterized by a strong cell-mediated immune response that limits bacterial growth and leads to localized granulomas and nerve damage, to a lepromatous form, with a weaker immune response that allows unrestricted bacterial proliferation, widespread skin lesions, and extensive nerve damage.
- Incubation period and chronicity: Mycobacterium leprae has an exceptionally long incubation period, ranging from months to several years. During this time, the bacteria multiply slowly within the host, often going unnoticed. The chronic nature of the disease is due to the bacterium’s slow growth rate and its ability to evade the immune system’s clearance mechanisms.
- Tissue damage and clinical manifestations: As Mycobacterium leprae continues to multiply within the host cells, it causes progressive damage to the skin, peripheral nerves, and other affected tissues. The clinical manifestations of leprosy include skin lesions, loss of sensation, muscle weakness, and deformities in advanced cases.
Lab Diagnosis
The laboratory diagnosis of Mycobacterium leprae involves various methods to detect the presence of the bacterium in clinical samples. Since it cannot be cultured in artificial laboratory media, the diagnosis mainly relies on microscopic examination, molecular techniques, and histopathological studies. Some of the common methods used for the lab diagnosis of Mycobacterium leprae are:
- Acid-fast staining: Acid-fast staining is a simple and rapid method used to visualize Mycobacterium leprae in clinical specimens. The Ziehl-Neelsen stain or the Kinyoun stain is commonly employed for this purpose. The clinical samples most commonly used for staining include slit-skin smears, skin biopsy specimens, or nasal smears. Acid-fast staining imparts a red color to acid-fast bacilli, including M. leprae, making them easily identifiable under a microscope.
- Slit-skin smears: Slit-skin smears are obtained by making superficial incisions or abrasions on skin lesions, and the exudates are collected and smeared onto a glass slide. These smears are then stained using acid-fast staining and examined under a microscope for the presence of Mycobacterium leprae.
- Skin biopsies: Skin biopsies from affected areas are taken for histopathological examination. The biopsy samples are processed, and sections are stained using the Ziehl-Neelsen stain or other specialized stains like Fite-Faraco stain to visualize the acid-fast bacilli within the tissues.
- Molecular methods: Polymerase chain reaction (PCR) is a highly sensitive and specific molecular technique used to detect the DNA of Mycobacterium leprae in clinical samples. PCR can be performed on slit-skin smear samples, skin biopsies, or nasal swabs. This method allows for early detection and differentiation of Mycobacterium leprae strains.
- Nerve biopsy: In cases of suspected leprosy involving nerve damage, nerve biopsies may be performed. The nerve tissues are processed and stained for acid-fast bacilli using histopathological methods.
It’s crucial to note that the diagnosis of leprosy is not solely based on the presence of Mycobacterium leprae in clinical samples. The clinical presentation, characteristic skin lesions, and neurological findings are also considered during the diagnosis. Furthermore, leprosy can present in different clinical forms, such as tuberculoid leprosy and lepromatous leprosy, which can have distinct histopathological features.
Treatment
The treatment of Mycobacterium leprae infection, commonly known as leprosy or Hansen’s disease, involves the use of multi-drug therapy (MDT). MDT is a combination of specific antibiotics that target the bacterium and help cure the infection. The World Health Organization (WHO) recommends MDT as the standard treatment for leprosy, and it has been highly successful in controlling and curing the disease.
The drugs used in multi-drug therapy for leprosy are as follows:
- Rifampicin: Rifampicin is a bactericidal antibiotic that is highly effective against M. leprae. It acts by inhibiting bacterial RNA synthesis, leading to the death of the bacteria. Rifampicin is one of the key drugs used in the initial phase of treatment.
- Dapsone: Dapsone is another bactericidal antibiotic used in MDT. It inhibits bacterial folic acid synthesis, resulting in bacterial death. Dapsone is administered in combination with rifampicin during the initial phase of treatment.
- Clofazimine: Clofazimine is a bacteriostatic antibiotic that inhibits bacterial growth. It is used in the later phase of MDT and helps prevent relapse of the disease. Clofazimine has anti-inflammatory properties and contributes to reducing the reactional episodes that can occur during treatment.
The duration of MDT depends on the type of leprosy and the severity of the infection. For paucibacillary (PB) leprosy, which has a low bacterial load, a six-month MDT regimen is prescribed, consisting of rifampicin and dapsone. For multibacillary (MB) leprosy, which has a higher bacterial load, a 12-month MDT regimen is recommended, consisting of rifampicin, dapsone, and clofazimine.
It’s essential for patients to complete the full course of treatment as prescribed by healthcare providers, even if they start feeling better before the treatment duration ends. This helps prevent the development of drug resistance and ensures complete eradication of the bacterium.
MDT has been highly effective in curing leprosy and preventing disabilities associated with the disease. With timely and appropriate treatment, most patients can be completely cured of leprosy, and the transmission of the disease can be significantly reduced.
Additionally, supportive care, wound care, and rehabilitation services may be provided to manage any existing disabilities and help affected individuals reintegrate into society. Early diagnosis and treatment remain crucial in achieving successful outcomes and preventing complications related to leprosy.
Prevention
Prevention of Mycobacterium leprae infection, commonly known as leprosy or Hansen’s disease, involves various strategies aimed at reducing transmission, early detection, and prompt treatment. While leprosy can be challenging to eradicate completely, these preventive measures can significantly reduce the burden of the disease:
- Early diagnosis and treatment: Early detection of leprosy cases and timely initiation of multi-drug therapy (MDT) are crucial in preventing the spread of the disease and minimizing complications. Healthcare providers, community health workers, and the public should be educated about the signs and symptoms of leprosy to ensure early identification and referral for treatment.
- Contact tracing and screening: Identifying and screening individuals who have been in close contact with confirmed leprosy patients can help detect and treat new cases early. Household and social contacts of leprosy patients should be examined for signs of the disease, especially if they have had prolonged exposure to the patient.
- Mass drug administration (MDA): In some high-burden areas, where leprosy is endemic, the World Health Organization (WHO) recommends targeted MDA as a preventive strategy. MDA involves providing a single dose of MDT to all individuals living in the affected community, regardless of whether they have active signs of leprosy. This approach aims to reduce the number of asymptomatic carriers and interrupt transmission.
- Health education and awareness: Raising public awareness about leprosy, its transmission, and early signs can help reduce stigma and discrimination associated with the disease. Educating communities about the availability of free treatment and the importance of early diagnosis can encourage affected individuals to seek help promptly.
- Improving living conditions: Overcrowded and unsanitary living conditions can facilitate the transmission of leprosy. Efforts to improve housing, sanitation, and access to clean water can help reduce the risk of infection.
- Strengthening healthcare services: Enhancing healthcare infrastructure and access to healthcare services in endemic areas can lead to early detection and treatment of leprosy cases. This includes training healthcare workers to recognize leprosy symptoms, provide timely treatment, and manage complications.
- Active case finding: Engaging in active case finding campaigns to screen high-risk populations, such as individuals living in leprosy-endemic regions or those with a family history of leprosy, can help identify and treat new cases early.
- Research and surveillance: Ongoing surveillance of leprosy cases helps monitor the disease’s prevalence, trends, and geographic distribution. Research efforts to understand the transmission dynamics and risk factors can inform more effective preventive strategies.
Keynotes
Here are key points to remember about Mycobacterium leprae:
- Mycobacterium leprae is the bacterium responsible for causing leprosy or Hansen’s disease, an ancient chronic infectious disease that primarily affects the skin and peripheral nerves.
- Morphology: M. leprae is a rod-shaped bacterium with a small size (1-8 micrometers in length) and acid-fast staining properties due to its high lipid content in the cell wall.
- Pathogenicity: M. leprae is an obligate intracellular pathogen, mainly infecting macrophages, Schwann cells, and endothelial cells. It has a slow growth rate and a long incubation period (months to years).
- Transmission: Leprosy is transmitted through respiratory droplets when an infected person coughs or sneezes. The majority of people have natural immunity, and not all exposed individuals develop the disease.
- Clinical forms: Leprosy can present in different clinical forms, ranging from tuberculoid leprosy (milder) to lepromatous leprosy (severe), depending on the host’s immune response.
- Laboratory diagnosis: Diagnosis is based on various methods, including acid-fast staining of slit-skin smears and skin biopsies, molecular techniques (PCR), and histopathological examination of affected tissues.
- Treatment: The standard treatment for leprosy is multi-drug therapy (MDT), which combines antibiotics like rifampicin, dapsone, and clofazimine. Early diagnosis and complete treatment are essential to prevent complications and disabilities.
- Prevention: Preventive measures include early diagnosis and treatment, contact tracing, screening, mass drug administration (MDA), health education, and improving living conditions.
- Global efforts: The World Health Organization (WHO) has made significant progress in controlling leprosy through global initiatives, aiming to eliminate leprosy as a public health problem.
- Stigma and discrimination: Leprosy has been historically associated with social stigma and discrimination. Raising awareness and education can help combat misconceptions and improve the lives of affected individuals.
Further Readings
- “Hansen’s Disease (Leprosy)” – World Health Organization (WHO) Website: https://www.who.int/health-topics/leprosy
- “Leprosy (Hansen Disease)” – Centers for Disease Control and Prevention (CDC) Website: https://www.cdc.gov/leprosy/index.html
- “Leprosy: Re-emergence of a forgotten disease” – PNAS (Proceedings of the National Academy of Sciences) Article: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4792522/
- “Epidemiology of leprosy” – Indian Journal of Dermatology, Venereology and Leprology Article: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2786561/
- “Leprosy in the 21st century” – Clinical Microbiology Reviews Article: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2772353/
- “Leprosy: A primer” – BMJ Global Health Article: https://gh.bmj.com/content/2/4/e000325
- “Leprosy: Current status and future challenges” – Indian Journal of Dermatology Article: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2888325/
- “Leprosy: Ancient Disease Remains a Public Health Problem Today” – National Institutes of Health (NIH) Website: https://www.niaid.nih.gov/diseases-conditions/leprosy-ancient-disease-remains-public-health-problem-today
- “Leprosy and the Immune Response” – Microorganisms Article: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7468716/