
Introduction of Rapid Plasma Reagin (RPR) Test
Table of Contents
RPR is a screening non-specific test for syphilis caused by a bacterium, Treponema pallidum. It has replaced the VDRL test due to having properties like no need of preparing fresh reagents daily, no need for a microscope, and also no need for heat inactivation of the serum sample. RPR assay works on the principle of flocculation and flocculation is a special type of precipitation where precipitates remain suspended instead of sedimentation.
Principle of RPR Test
In the RPR test, the RPR antigen is mixed with unheated or heated serum or with unheated plasma on a plastic-coated card. The reagin binds to the test antigen which consists of cardiolipin-lecithin coated particles that cause macroscopic flocculation resulting in aggregation of carbon particles. The flocculation appears as black clumps against the white background of the plastic-coated card. The RPR test measures IgM and IgG antibodies to lipoidal material released from damaged host cells as well as to lipoprotein-like material, and possibly cardiolipin released from the treponemes.
Antilipoidal antibodies are antibodies that are produced not only as a consequence of syphilis and other treponemal diseases but also in response to nontreponemal diseases of an acute and chronic nature in which tissue damage occurs. The antigen is prepared from a modified Venereal Disease Research Laboratory (VDRL) antigen suspension containing choline chloride to eliminate the need to heat inactivate serum, ethylenediaminetetraacetic acid (EDTA) to enhance the stability of the suspension, and finely divided charcoal particles as a visualizing agent.
Test Requirements for RPR test
Test requirements for the assay are as follows-
- Test Specimens: Serum /Plasma
- Test Reagents
- RPR antigen suspension:- stabilized combination of 0.003% cardiolipin, 0.020-0.022% lecithin, 0.09% cholesterol, 10% choline chloride, 0.0125M EDTA, 0.01875% charcoal, 0.01M Na2HP04, 0.01M KH2P04, 0.1% thimerosal in distilled water.
- Control serum samples:– Control serum samples are lyophilized reactive (R), minimally reactive (Rm), and nonreactive (N) control serum specimens.
- 0.9% Saline:- Add 0.9 g of dry sodium chloride (ACS) to 100 ml of distilled water. Disposable, calibrated 20-gauge needle without bevel.
Others
- Plastic antigen dispensing bottle
- Plastic-coated RPR cards, with 10 circles, each approximately 18 mm in diameter.
- Mechanical rotator, fixed-speed or adjustable to 100 + 2 rpm
- High-intensity incandescent lamp
- Safety pipetting device with a disposable tip that delivers 50 μl
The procedure of the RPR Test
RPR Qualitative Test
Place 50 μl of serum or plasma onto an 18-mm circle of the RPR test card. Using the inverted Dispenstir (closed-end) or flat toothpicks, spread the serum or plasma to fill the entire circle. Do not spread the specimen beyond the confines of the circle. Gently shake the antigen dispensing bottle to resuspend the particles. Holding the dispensing bottle and needle in a vertical position, exactly 1 free-falling drop (17 μl) of antigen suspension to each circle containing serum or plasma. Do not mix. Place the card on the mechanical rotator under a humidifying cover. Rotate the card for 8 minutes at 100 + 2 rpm. Immediately remove the card from the rotator; briefly rotate and tilt the card by hand (three or four to-and-fro motions) to aid in differentiating nonreactive from minimally reactive results)
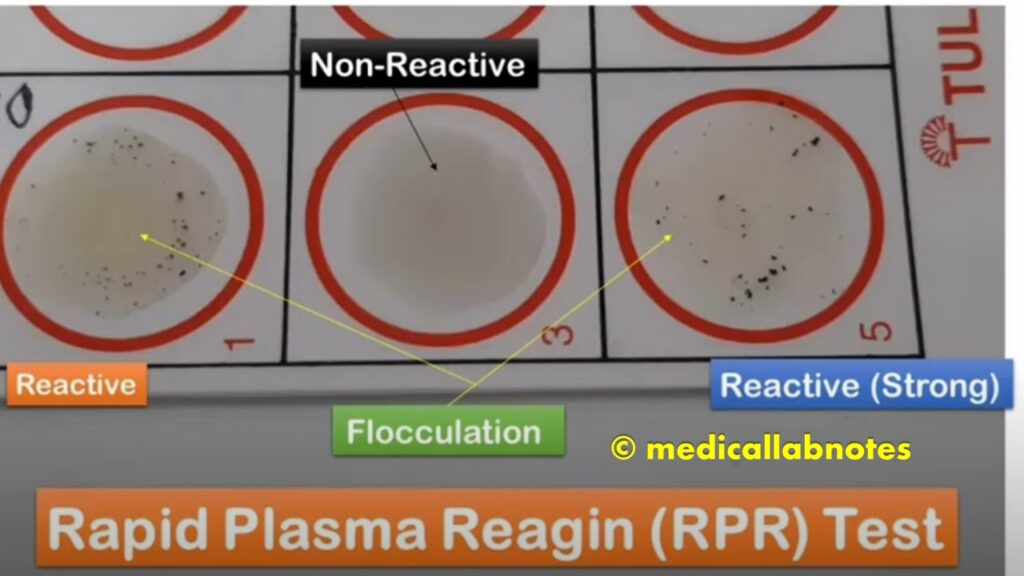
Reading and Reporting Qualitative RPR test Results
Read the test reactions under a high-intensity incandescent lamp.
Reading Report-
| Observation | Report |
| Characteristic clumping ranges from marked and intense (reactive) to slight but definite (minimally to moderately reactive) | Reactive (R) |
| Slight roughness or no clumping | Non-reactive (N) |
RPR Quantitative Test
Dilute to an endpoint titer all serum specimens with rough nonreactive results in the qualitative test. Test each specimen undiluted (1:1), and in 1:2, 1:4, 1:8, and 1:16 dilutions. Place 50 μl of 0.9% saline in circles numbered 2 through 5. Do not spread the saline. Using a safety pipette device, place 50 μl of serum in circle 1 and 50 μl of serum in circle 2.
Mix the saline and the serum in circle 2 by drawing the mixture up and down in a safety pipette eight times. Transfer 50 μl from circle 2 (1:2) to circle 3, and mix.Transfer 50 μl from circle 3 (1:4) to circle 4, and mix. Transfer 50 μl from circle 4 (1:8) to circle 5 (1:16), mix, and then discard the last 50 μl. Proceed as RPR qualitative test. If reactive at the last dilution further dilute the serum and test.After completing the day’s tests, remove the needle from the antigen dispensing bottle. Rinse the needle in distilled water, and air dry. Reading and Reporting quantitative results
Read the test reaction under a high-intensity incandescent lamp for the qualitative test.
Result- Interpretation
A reactive RPR card test may suggest past or present infection with a pathogenic treponeme; however, it may also be a false-positive reaction.
A nonreactive RPR card test without clinical evidence of syphilis may suggest no current infection or an effectively treated infection. A nonreactive test with clinical evidence of syphilis can be seen in early primary syphilis; secondary syphilis, as a result of the prozone reaction; and in some cases late syphilis. This nonreactive card test result does not rule out an incubating syphilis infection. When the quantitative RPR card test is performed on patients with syphilis, a fourfold rise in titer in a repeat specimen may suggest an infection, reinfection, or a treatment failure, a fourfold decrease, e.g. 1:16 to 1:4, in titer following treatment for early syphilis usually indicates that therapy was adequate.
All reactive qualitative RPR card tests should be diluted to an endpoint and the endpoint titer reported. Unusually high RPR card test titers can be seen with concurrent human immunodeficiency virus type 1 (HIV-1) infection. Unusually high false-positive titers may also be seen in patients with lymphomas.
Limitations of the Test
A prozone reaction may be encountered occasionally. The RPR card test may be reactive in persons from areas where yaws, pinta, or nonvenereal syphilis is endemic. Biological false-positive (BFP) reactions occur occasionally. Non-syphilitic conditions give biologic false-positive results in non-treponemal tests like malaria, leprosy, relapsing fever, infectious mononucleosis, atypical pneumonia, infectious hepatitis, and rheumatoid arthritis, pregnancy, aging individuals, viral pneumonia, lupus erythematous, measles, pregnancy, drug abuse, pneumococcal pneumonia, etc.
Keynotes
Qualitative RPR test Results-
False Negative Reactions
- Technical error – unsatisfactory antigen or technique
- Low antibody titers
- Presence of inhibitors in the patient’s serum
- Reduced ambient temperature (below 23°C to 29°C)
- Prozone reaction
Why VDRL is replaced by the RPR test?
Because of the following features-
- In the RPR test- There is no need of preparing fresh reagents daily.
- No need for a microscope
- No need for heat inactivation of the serum sample
- But one demerit of the RPR test- the CSF sample can not be tested.
Bibliography
- https://wwwn.cdc.gov/nchs/data/nhanes/20032004/labmethods/l36_c_met_rpr.pdf
- https://www.urmc.rochester.edu/encyclopedia/content
- https://www.ucsfhealth.org/medical-tests/003533
- https://www.medicinenet.com/script/main/art.asp?articlekey=9225
- Textbook of Medical Laboratory Technology by Praful B. Godkar, Darshan P. Godkar
- Textbook of Medical Laboratory Technology by Ramnik Sood (2006)
- http://www.arlingtonscientific.com/assets/rpr-clsi-document.pdf
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3312652/
- https://cmr.asm.org/content/cmr/8/1/1.full.pdf
- https://apps.who.int/iris/bitstream/handle/10665/262186/PMC2396117.pdf?sequence=1&isAllowed=y
- https://www.hindawi.com/journals/jir/2018/2978419/