
Introduction
Table of Contents
Nocardia is a genus of aerobic, gram-positive bacteria. It belongs to the actinomycetes group. These bacteria are partially acid-fast due to mycolic acid in their cell walls. They commonly appear as branching filamentous rods. Nocardia species are found in soil and water. They can cause infections in humans and animals. Nocardiosis, the infection caused by Nocardia, primarily affects the lungs, brain, and skin. People with weakened immune systems are at higher risk. Symptoms vary based on the infection site. Pulmonary nocardiosis can mimic tuberculosis. Cutaneous infections often result from traumatic injuries. Diagnosis involves culture, staining, and molecular methods. Treatment typically requires prolonged antibiotic therapy. Nocardia species are resistant to many antibiotics, necessitating susceptibility testing. Proper identification and management are crucial for effective treatment. Researchers and clinicians continue to study Nocardia to improve diagnosis and treatment strategies.
Morphology
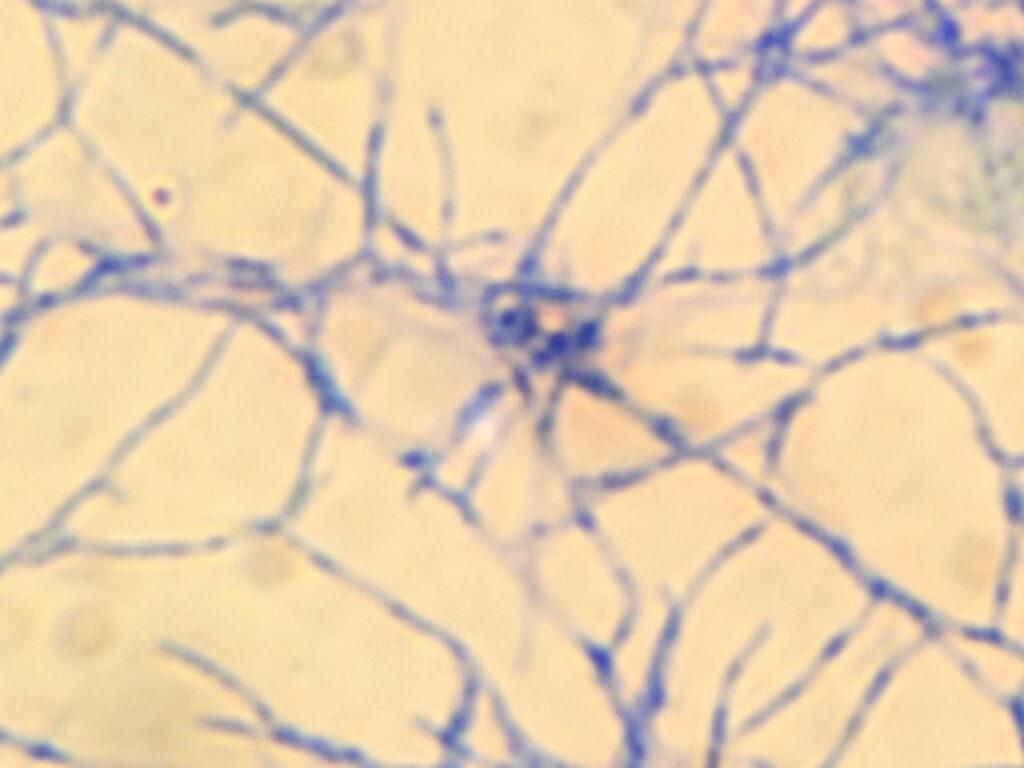
Nocardia bacteria are gram-positive and partially acid-fast. They appear as branching filamentous rods. These bacteria can form aerial hyphae. Nocardia species have a beaded appearance under the microscope. The cells range from 1 to 2 micrometers in diameter. Colonies on agar are often chalky and white. They can also be orange or pink. The colonies have a dry and wrinkled texture. Nocardia‘s branching structure resembles fungal hyphae.

This morphology helps differentiate them from other bacteria. Proper staining techniques highlight their unique structure. The distinct morphology aids in identification and diagnosis.

Pathogenicity
Nocardia is a significant pathogen, especially in immunocompromised individuals. It causes nocardiosis, a serious infection. Pulmonary nocardiosis is the most common form. It can mimic tuberculosis or pneumonia. Nocardia can spread from the lungs to the brain, causing brain abscesses. Cutaneous nocardiosis results from traumatic injuries. Skin infections can lead to chronic ulcers or abscesses. It can also infect the central nervous system. The bacteria can disseminate to other organs, complicating treatment. Nocardia‘s pathogenicity is due to its ability to survive within macrophages. This evasion of the immune system makes it hard to treat. Resistance to many antibiotics is common. Therefore, accurate identification and susceptibility testing are crucial. Prolonged antibiotic therapy is often necessary. Without proper treatment, nocardiosis can be fatal. Early diagnosis improves patient outcomes significantly. Researchers continue to study Nocardia to develop better treatments. Understanding its pathogenicity helps in managing infections effectively.
Lab Diagnosis
Lab diagnosis of Nocardia involves multiple steps to ensure accurate identification. First, collect appropriate clinical specimens. These include sputum, pus, or tissue biopsies. Use aseptic techniques to avoid contamination. Gram staining is the initial step. Nocardia appears as gram-positive, branching filamentous rods. Next, perform a modified acid-fast stain. It shows partial acid-fastness, appearing red against a blue background. Culture the specimens on suitable media. Use Sabouraud Dextrose Agar (SDA) or Lowenstein-Jensen (LJ) medium. Incubate the cultures at 35-37°C for 1-2 weeks. Nocardia colonies are dry, chalky, and white or pigmented.

Observation of aerial hyphae helps differentiate Nocardia from other actinomycetes. Perform biochemical tests to identify the species further. Nocardia species are typically urease and nitrate reduction positive. Molecular methods, like PCR, offer precise identification. Use 16S rRNA sequencing for species-level identification. Mass spectrometry (MALDI-TOF MS) can also identify Nocardia quickly. Antibiotic susceptibility testing is crucial due to Nocardia’s resistance patterns. Use broth microdilution or E-test methods for accurate results.

Direct fluorescent antibody testing provides rapid identification of clinical samples. Regular observation and documentation of colony morphology are important. Compare the growth with control organisms if needed. Proper lab safety protocols must be followed due to the pathogenic nature of Nocardia. Dispose of biohazard waste according to guidelines.

Accurate lab diagnosis is essential for effective treatment. Early and precise identification improves patient outcomes. Combining different diagnostic methods enhances the reliability of Nocardia identification. Researchers continue to refine diagnostic techniques for better accuracy.

Treatment
Treatment of Nocardia infections requires prolonged antibiotic therapy. Sulfonamides, especially trimethoprim-sulfamethoxazole, are the first-line treatment. Doctors often use a combination of antibiotics. Amikacin, imipenem, and linezolid are common choices. Treatment duration typically ranges from six months to a year. Severe cases may need intravenous antibiotics initially. Always perform antibiotic susceptibility testing to guide therapy. Adjust treatment based on the patient’s response and test results. Monitor patients closely for side effects. Surgical intervention may be necessary for abscess drainage. Early and accurate diagnosis improves treatment outcomes significantly. Regular follow-up is essential to ensure complete resolution of the infection.
Prevention
Preventing Nocardia infections involves several strategies. Immunocompromised individuals should take extra precautions. Avoid activities that expose you to soil and dust. Wear protective clothing and masks when gardening or working with soil. Proper wound care is essential to prevent skin infections. Clean cuts and abrasions immediately with antiseptic solutions. Cover wounds with sterile dressings until they heal. Regularly clean and disinfect living areas. Avoid exposure to contaminated water sources. Healthcare workers should follow strict infection control protocols. Use sterile techniques when handling clinical specimens. Implement environmental controls in hospital settings. Educate at-risk patients about the signs of nocardiosis.

Early recognition of symptoms aids in prompt treatment. Encourage regular medical check-ups for high-risk individuals. Maintaining a strong immune system helps reduce infection risk. Consume a balanced diet, exercise regularly, and manage chronic conditions effectively. Avoid unnecessary use of immunosuppressive drugs. Research and public health measures continue to play a role in prevention. Public awareness campaigns can help reduce the incidence of Nocardia infections.
Keynotes
Nocardia is a genus of gram-positive, aerobic bacteria. It belongs to the actinomycetes group and is partially acid-fast. These bacteria appear as branching filamentous rods. Found in soil and water, Nocardia causes infections mainly in immunocompromised individuals. Nocardiosis affects the lungs, brain, and skin. In particular, pulmonary nocardiosis mimics tuberculosis or pneumonia. Moreover, skin infections occur through traumatic injuries. Additionally, the bacteria can spread, causing systemic infections. Diagnosis involves Gram staining, acid-fast staining, and culture. Nocardia grows on Sabouraud Dextrose Agar and Lowenstein-Jensen medium. Colonies are dry, chalky, and white or pigmented. Furthermore, molecular methods like PCR and 16S rRNA sequencing offer precise identification.
Treatment requires prolonged antibiotic therapy. Trimethoprim-sulfamethoxazole is the first-line treatment. Besides, other antibiotics include amikacin, imipenem, and linezolid. Consequently, antibiotic susceptibility testing guides therapy. Preventing infections involves avoiding exposure to soil and dust. Therefore, proper wound care is crucial. Immunocompromised individuals should take extra precautions. In healthcare settings, workers must follow infection control protocols. Early diagnosis and treatment improve outcomes significantly. Nocardia‘s pathogenicity is due to its ability to evade the immune system. Research continues to develop better diagnostic and treatment methods. Hence, public awareness helps reduce infection rates.


Further Readings
- https://www.cdc.gov/nocardiosis/about/index.html
- https://www.sciencedirect.com/topics/medicine-and-dentistry/nocardia
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC254378/
- https://www.uptodate.com/contents/treatment-of-nocardiosis
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9127990/
- https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-021-06416-w
- https://journal.chestnet.org/article/S0012-3692(18)31357-6/fulltext
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10080825/
- https://casereports.bmj.com/content/13/12/e237208