
Introduction
Table of Contents
Acinetobacter baumannii is a Gram-negative, non-fermenting, aerobic coccobacillus. It is an opportunistic pathogen increasingly associated with nosocomial infections, particularly in critically ill or immunocompromised patients. Notorious for its antibiotic resistance, it has become a major global health concern, particularly in ICU settings.
Morphology
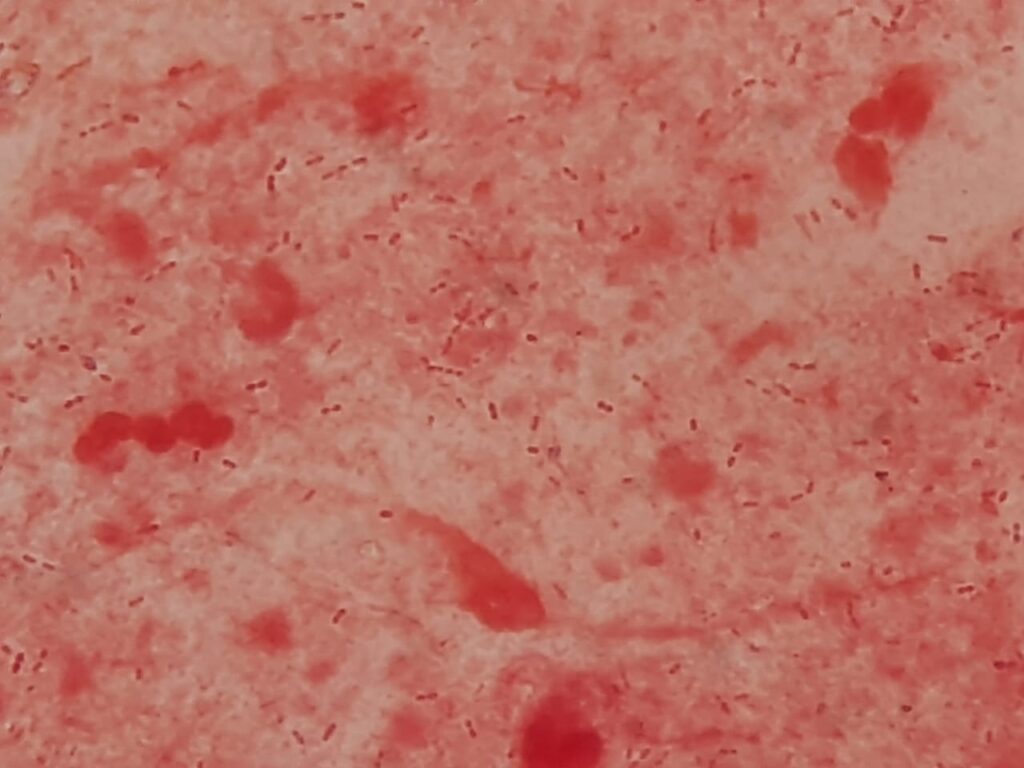
- Gram-negative coccobacilli, often appearing in pairs
- Non-motile, oxidase-negative, and catalase-positive
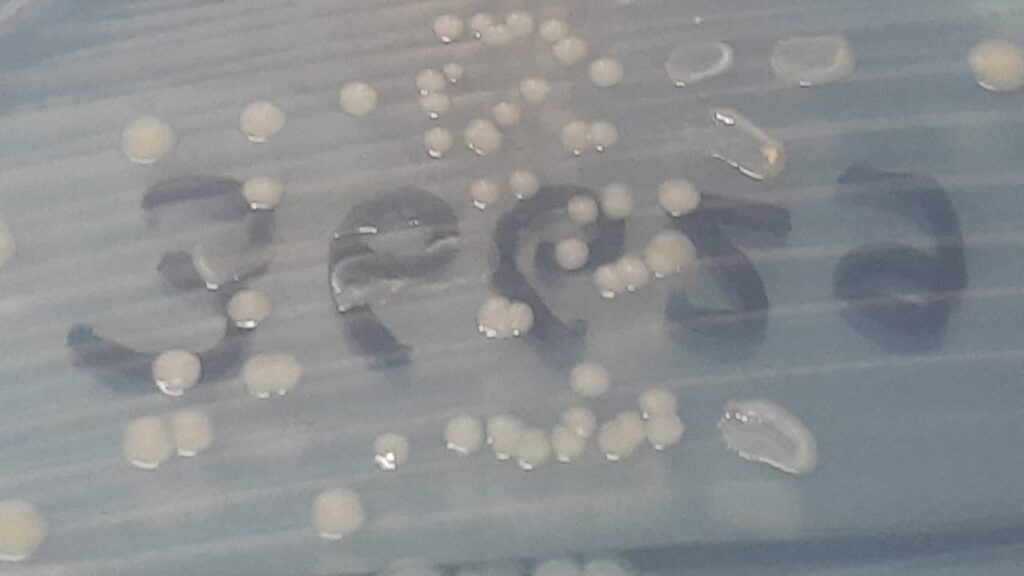
- Appears as smooth, opaque, creamy colonies on blood agar
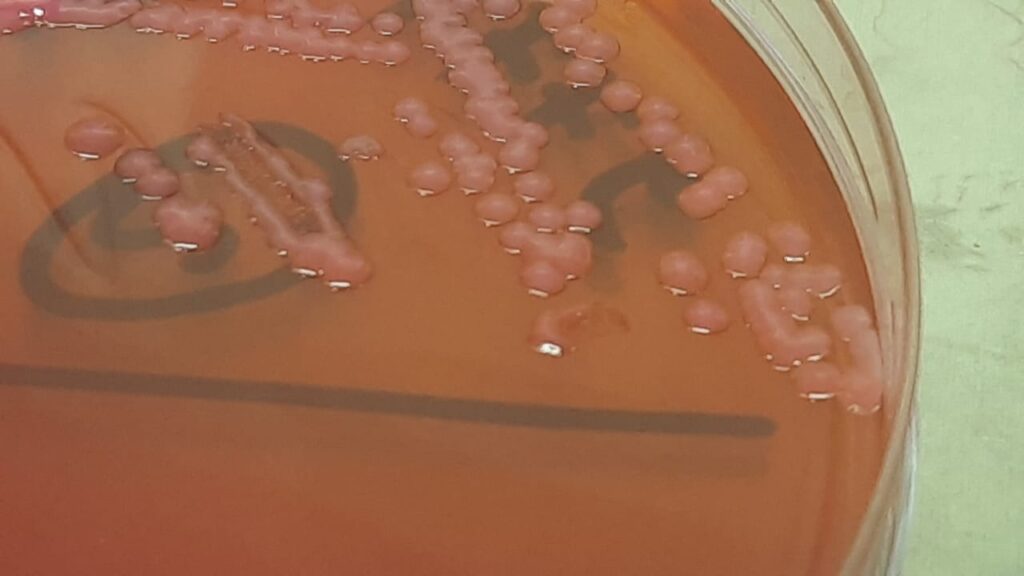
- Non-lactose fermenting on MacConkey agar
- Survives for long periods on surfaces due to desiccation resistance

Pathogenicity
- Causes ventilator-associated pneumonia (VAP), bloodstream infections (BSI), meningitis, wound infections, and urinary tract infections (UTIs)
- Produces biofilms, contributing to device-related infections
- Secretes enzymes such as β-lactamases and has efflux pumps
- Known for horizontal gene transfer, contributing to multidrug resistance (MDR)
- Targets include patients with catheters, ventilators, open wounds, or prolonged antibiotic exposure
{kind=link}
Laboratory Diagnosis
- Specimens: Sputum, blood, CSF, urine, wound swabs
- Culture characteristics:
- Growth on blood agar and MacConkey agar (non-lactose fermenter)
- Microscopy: Gram stain shows Gram-negative coccobacilli
- Biochemical tests:
- Oxidase-negative
- Non-fermenter in oxidative-fermentative media
- Advanced ID methods:
- MALDI-TOF MS, VITEK, or PCR for species confirmation
- Antimicrobial susceptibility testing (AST):
- Essential due to frequent MDR/XDR profiles

Treatment
- Empirical therapy should be guided by the local antibiogram
- MDR strains are often resistant to carbapenems, cephalosporins, and aminoglycosides
- Commonly used antibiotics:
- Colistin (polymyxin E)
- Tigecycline
- Minocycline
- Cefiderocol
- High-dose sulbactam
- Combination therapy may be considered for XDR strains
- Avoid unnecessary antibiotics to reduce pressure
Prevention
- Hand hygiene and contact precautions in hospitals
- Environmental cleaning and disinfection
- Surveillance of ICU and high-risk wards
- Isolation or cohorting of infected patients
- Antimicrobial stewardship to prevent resistance emergence
- Regular monitoring of device-related infections (e.g., catheters, ventilators)
Keynotes
- Acinetobacter baumannii is a critical priority pathogen (WHO list) due to MDR/XDR resistance
- Commonly associated with ICU outbreaks
- Has high environmental resilience, surviving on dry surfaces for weeks
- Accurate identification and susceptibility testing are crucial
- Treatment options are limited, and resistance is rising
- Prevention and strict infection control measures are vital
Further Readings
- https://pmc.ncbi.nlm.nih.gov/articles/PMC3442836/
- https://www.cdc.gov/acinetobacter/about/index.html
- https://gardp.org/stories/meet-acinetobacter-baumannii/
- https://academic.oup.com/femspd/article/71/3/292/475786
- https://www.webmd.com/a-to-z-guides/what-to-know-about-acinetobacter-baumannii
- https://www.msdmanuals.com/professional/infectious-diseases/gram-negative-cocci-and-coccobacilli/acinetobacter-infections
- https://www.nature.com/articles/nrmicro1789
- https://journals.asm.org/doi/10.1128/cmr.00058-07
- https://web.sanfordguide.com/e1f1b28667ed4739a3c5cd85dc24f64f