
Introduction
Table of Contents
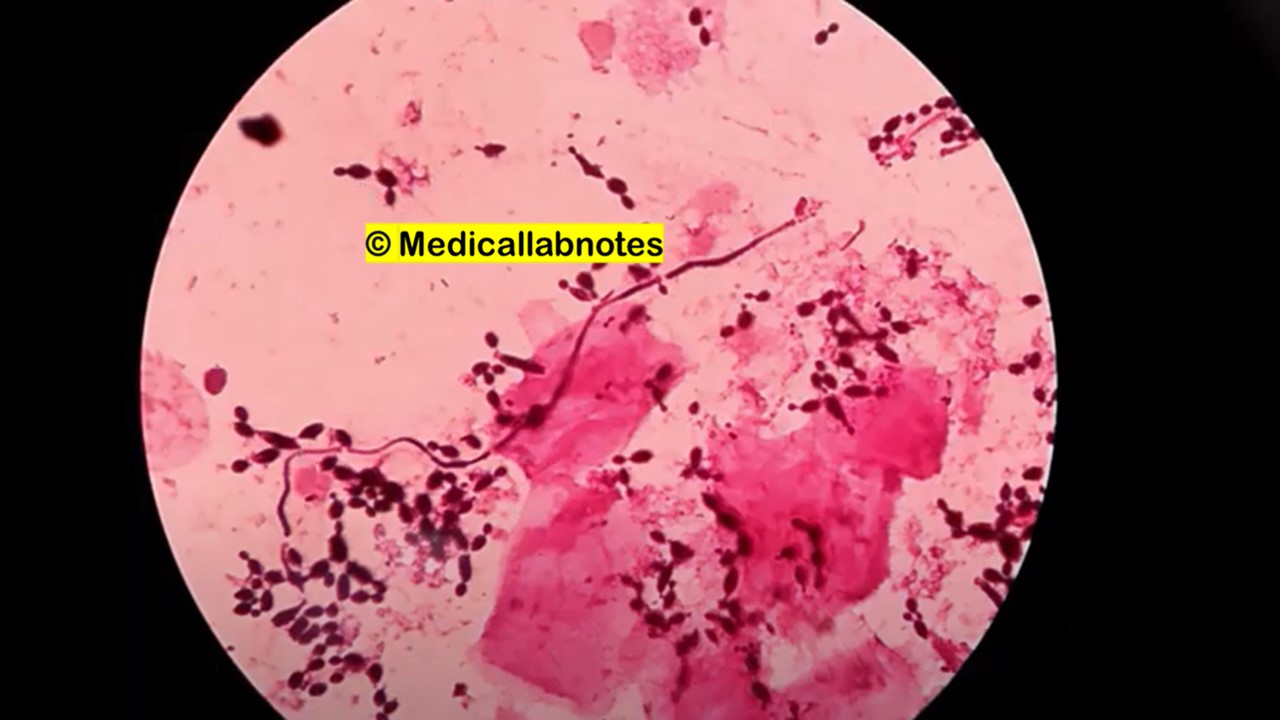
Funguria refers to the presence of fungi in the urine, either due to colonization, contamination, or true urinary tract infection (UTI).

It is increasingly reported in hospitalized or catheterized patients, particularly those with immunosuppression, antibiotic overuse, or diabetes. Most cases are asymptomatic, but it can lead to pyelonephritis, fungal balls, or sepsis, especially in neonates and ICU patients.
Common Fungi Causing Funguria
| Fungal Pathogen | Notes |
|---|---|
| Candida albicans | Most common; forms pseudohyphae |
| Candida glabrata | Second most common; less susceptible to azoles |
| Candida tropicalis | Associated with hematologic malignancy |
| Candida krusei | Intrinsically resistant to fluconazole |
| Candida parapsilosis | Catheter-associated funguria |
| Cryptococcus neoformans | Rare; may be seen in AIDS or renal transplant |
| Aspergillus spp. | Very rare; usually from contamination or systemic spread |
Clinical Features
- Most patients are asymptomatic.
- When symptomatic:
- Dysuria, frequency, urgency
- Flank pain, fever, chills
- Cloudy or foul-smelling urine
- Fungal balls may obstruct the urinary tract in neonates or catheterized patients
- In cryptococcal funguria, symptoms may be minimal or absent
Laboratory Diagnosis
| Test | Purpose |
|---|---|
| Direct Microscopy (Wet mount/KOH) | Detect yeast cells, pseudohyphae |
| Urine Gram stain | May reveal budding yeast |
| Urine Culture (SDA, CHROMagar Candida) | Confirm fungal growth; >10⁴–10⁵ CFU/mL significant |
| Repeat Culture | Helps differentiate colonization vs infection |
| Blood culture | Rule out disseminated candidiasis in high-risk cases |
| Urinalysis | Pyuria may be present; may also be sterile |
| Ultrasound/CT Scan | Detect fungal balls or obstruction in complicated cases |
{kind=link}







Treatment
| Indication | Treatment |
|---|---|
| Asymptomatic, low-risk patient | No treatment; remove catheter if possible |
| Symptomatic infection | Fluconazole is first-line if susceptible |
| Fluconazole-resistant strains | Use Amphotericin B deoxycholate bladder irrigation or systemic Echinocandins |
| Obstructing fungal balls | Surgical removal + antifungals |
| Cryptococcal funguria | Treat as disseminated cryptococcosis: Amphotericin B ± Flucytosine |
Prevention
- Avoid unnecessary urinary catheters
- Minimize broad-spectrum antibiotic use
- Control diabetes mellitus
- Maintain good perineal hygiene
- Perform regular catheter care
- Screen high-risk ICU or post-op patients if symptomatic
- Use prophylactic antifungals in high-risk transplant or neutropenic patients selectively
Keynotes
- Funguria is mostly due to Candida spp., especially in catheterized and ICU patients.
- Asymptomatic cases often don’t require treatment unless risk factors exist.
- Diagnosis depends on culture, microscopy, and clinical correlation.
- Fluconazole remains the treatment of choice if the isolate is susceptible.
- Prevention relies on infection control, catheter care, and antibiotic stewardship.
Further Readings
- https://link.springer.com/article/10.1007/s003450050167
- https://www.sciencedirect.com/science/article/abs/pii/S0924857999000321
- https://www.merckmanuals.com/professional/genitourinary-disorders/urinary-tract-infections-utis/fungal-urinary-tract-infections
- https://journals.sagepub.com/doi/10.1177/08850666241231495
- https://pubmed.ncbi.nlm.nih.gov/11584989/
- https://www.urologic.theclinics.com/article/S0094-0143(24)00062-4/pdf
- https://www.auajournals.org/doi/pdf/10.1016/S0022-5347%2801%2967255-0
- https://academic.oup.com/cid/article/52/suppl_6/S437/284654
- https://www.urotoday.com/2014-09-18-02-47-34/infections-main/6523-genitourinary-fungal-infections-4949.html
- https://pubmed.ncbi.nlm.nih.gov/17544611/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC4277144/
- https://www.scielo.br/j/bjid/a/GYBZgBrQxBHTzFSw4NrMzdn/?lang=en
- https://www.baus.org.uk/_userfiles/pages/files/professionals/bsot/TJW-Funguria.pdf